Iron deficiency anemia as a risk factor for the first episode of febrile seizure
Saleem M.1, Ahmed Siddique A.2*
DOI: https://doi.org/10.17511/ijpr.2020.i02.08
1 Mohammed Abdul Saleem, Assistant Professor, Department of Paediatrics, Gandhi Medical College, Secunderabad, Telangana, India.
2* Abrar Ahmed Siddique, Assistant Professor, Department of Paediatrics, Niloufer Hospital, Hyderabad, Telangana, India.
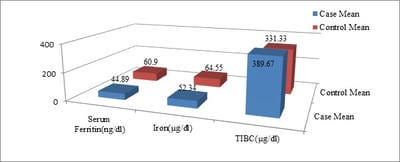
Background: Febrile seizures are defined as an event in neurologically healthy infants and children between 6 months and 5 years of age, associated with fever >38ºC rectal temperature but without evidence of intracranial infection as a defined cause and with no history of prior afebrile seizures. Objective: This study is aimed at evaluating the association between iron deficiency anemia and febrile seizures. Design: A prospective hospital-based study, carried out in the Department of Pediatrics, Gandhi Hospital, Secunderabad. Duration: October 2014 to November 2015. Setting: Department of Pediatrics, Gandhi Hospital, Secunderabad. Participants: 50 cases of the first episode of simple febrile seizure in the age group of 1 year to 5 years admitted to the pediatric ward. A control group was selected from age and sex-matched children admitted with febrile illness but without a seizure. Methods: Cases were patients with typical febrile convulsions between 1 year to 5 years (AAP clinical practice guidelines). In all cases, detailed clinical history, anthropometry, a clinical sign of iron deficiency, CNS examination was done. Hematological investigations including CBC, PBF, Red cell indices, Serum Iron, Serum Ferritin and Serum TIBC level were done. Results: Incidence of anemia among case group subjects was 88% whereas the same in the control group was 24%. Mean RDW and TIBC levels in cases were significantly higher as compared to that in controls. MCV, Mean Serum Ferritin and Serum Iron levels in cases were significantly lower as compared to that in controls. Conclusion: The findings suggest that a considerable percentage of children having febrile seizures suffer from iron-deficiency anemia and low serum iron. This means the low serum iron and the presence of anemia can serve as a reinforcing factor for febrile seizures in children.
Keywords: Febrile convulsions, Iron-deficiency Anemia, Children
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Assistant Professor, Department of Paediatrics, Niloufer Hospital, Hyderabad, Telangana, India. Email:  |
Saleem MA, Siddique AA. Iron deficiency anemia as a risk factor for the first episode of febrile seizure. Pediatric Rev Int J Pediatr Res. 2020;7(2):93-96. Available From https://pediatrics.medresearch.in/index.php/ijpr/article/view/578 |
 |
 ©
©