To study renal parameters and serum calcium levels in birth asphyxia
Patidar A.1, Chandra Mandliya J.2*, Sonker P.3, Dhaneria M.4
DOI: https://doi.org/10.17511/ijpr.2020.i06.06
1 Amit Patidar, PG Resident, Department of Pediatrics, R.D. Gardi Medical College, Ujjain, Madhya Pradesh, India.
2* Jagdish Chandra Mandliya, Professor, Department of Pediatrics, R.D. Gardi Medical College, Ujjain, Madhya Pradesh, India.
3 Pavan Sonker, Professor, Department of Biochemistry, R.D. Gardi Medical College, Ujjain, Madhya Pradesh, India.
4 Mamta Dhaneria, Head of Department and Professor, Department of Pediatrics, R.D. Gardi Medical College, Ujjain, Madhya Pradesh, India.
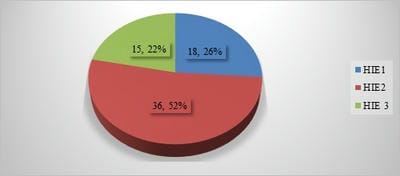
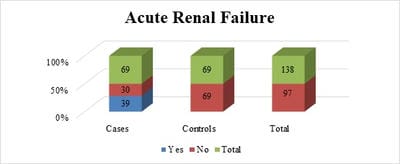
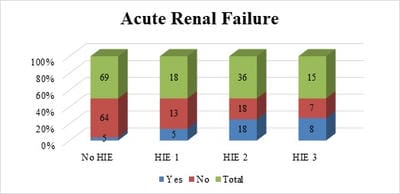
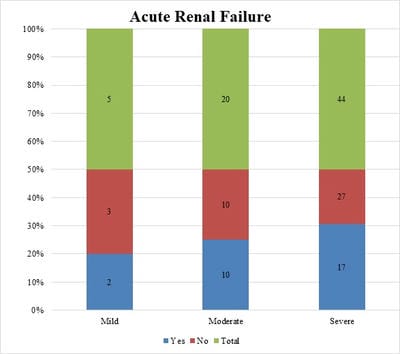
Background: Birth asphyxia is a common neonatal problem and contributes significantly to neonatal mortality and long term morbidity. Any organ can be affected but the brain, heart, kidneys are more sensitive to hypoxic injury. Aim and Objective: To study renal parameters and serum calcium levels in birth asphyxia, to determine the incidence of renal failure in asphyxiated newborns, and to correlate the renal parameters with different severity of birth asphyxia and with different stages of hypoxic-ischemic encephalopathy. Method and material: A comparative study of 69 term newborns, appropriate for gestational age born/admitted to tertiary care Centre RDGMC Ujjain with birth asphyxia and 69 normal newborns without birth asphyxia was done. Perinatal history, physical examinations, New Ballard score, Apgar score was done. Data collected and entered in the master chart for results and analysis. Result: The study included 69 cases and 69 controls with the majority of boys. Mild, moderate, and severe birth asphyxia was7%, 29%, and 64% of all cases respectively. The incidence of acute renal failure was 57% among cases of birth asphyxia. The incidence of acute renal failure was 53% and 50% in hypoxic-ischemic encephalopathy stages III and II respectively. Incidence of renal failure with mild, moderate, and severe asphyxia was 40%, 50%, and 39% respectively Conclusion: Perinatal asphyxia is an important cause of neonatal renal failure. Monitoring of urea, creatinine and urine output helps in the early diagnosis and management of acute renal failure
Keywords: Acute Renal failure, Birth asphyxia, Hypoxic Ischemic Encephalopathy (HIE), Sarnat and Sarnat Staging
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Professor, Department of Pediatrics, R.D. Gardi Medical College, Ujjain, Madhya Pradesh, India. Email:  |
Patidar A, Mandliya JC, Sonker P, Dhaneria M. To study renal parameters and serum calcium levels in birth asphyxia. Pediatric Rev Int J Pediatr Res. 2020;7(6):255-261. Available From https://pediatrics.medresearch.in/index.php/ijpr/article/view/611 |
 |
 ©
©