Assessment of the nutritional status of adolescent girls aged between 15 to 18 years studying in government high school in Raipur, Chhattisgarh, India
Phuljhele S.1, Dewangan S.2, A.3*
DOI: https://doi.org/10.17511/ijpr.2021.i02.06
1 Sharja Phuljhele, Professor and HOD, Department of Paediatrics, Pt. JNM Medical College, Raipur, Chhattisgarh, India.
2 Shashikant Dewangan, Assistant Professor, Department of Paediatrics, Pt. JNM Medical College, Raipur, Chhattisgarh, India.
3* Anu , Postgraduate, Department of Paediatrics, Pt. JNM Medical College, Raipur, Chhattisgarh, India.
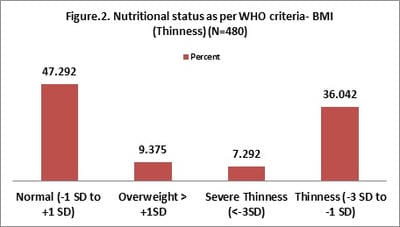
Introduction: The prevalence of malnutrition among adolescent girls is high in India. Malnutrition has long term effects on the physical and mental health of adolescents. Objectives: To find out the prevalence of underweight, overweight and stunting and correlate with a dietary pattern, socio-demographic profile and prevalence of clinical anemia and signs of vitamin and mineral deficiency. Method: This is a community-based cross-sectional observational study conducted for 1 year (Jan 2019 – Dec 2019), including a total of 480 adolescent girls who were attending government high school. Observations and Result: 480 girls were interviewed. As per WHO nutritional measurement criteria, adolescent girls were classified as per their anthropometric criteria, 50.63% of girls were moderately stunted and 7.29% had severe stunting. 7.29% of girls were in the category of severe thinness, 36.04% had thinness and 9.37% were overweight. 28.12% had conjunctival pallor (anaemia), 4.80% had dental caries, 1.46% had vitamin B complex deficiency and 1.04% had signs of vitamin A deficiency. Conclusion: More than half of the (57.92%) late adolescent school girls were stunted, 43.33% were having some form of thinness and 28.12% had clinical anaemia. Effective implementation of government programs such as the RKSK and Sabla Yojana program will be a paradigm shift from the existing clinic-based services to promotion and prevention and reaching adolescents in their environment, such as in schools, families and communities. Skills-based nutrition education for the family and effective infection control and routine health assessment of school-going girls should be done.
Keywords: Adolescent girls, Government high schools, Nutritional status
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Postgraduate, Department of Paediatrics, Pt. JNM Medical College, Raipur, Chhattisgarh, India. Email:  |
Phuljhele S, Dewangan S, Anu. Assessment of the nutritional status of adolescent girls aged between 15 to 18 years studying in government high school in Raipur, Chhattisgarh, India. Pediatric Rev Int J Pediatr Res. 2021;8(2):100-108. Available From https://pediatrics.medresearch.in/index.php/ijpr/article/view/671 |
 |
 ©
©