TumsUP Drops: Evaluation of safety and efficacy in infantile colic.
Dewan B.1*, Shinde S.2
DOI: https://doi.org/10.17511/ijpr.2023.i01.02
1* Bhupesh Dewan, MBBS, MD (Pharmacology), Director, Department of Medical Services, Zuventus Healthcare Limited, Mumbai, Maharashtra, India.
2 Siddheshwar Shinde, M. Pharm (Pharmacology), Manager, Department of Medical Services, Zuventus Healthcare Limited, Mumbai, Maharashtra, India.
Objectives: This study aimed to evaluate the safety and efficacy of TumsUP drops in the treatment of infantile colic in infants and toddlers. Setting and Design: An active post-marketing surveillance study was conducted in the department of pediatrics of 4 hospitals from August 2020 to February 2021. Material and Methods: A total of 200 patients aged two weeks to two years, with symptoms of infantile colic for >3 hours/day, occurring >3 days/week were enrolled. TumsUP (A fixed-dose combination of simethicone 40 mg, dill oil 0.005 mL, and fennel oil 0.0007 mL) oral drops were administered for 7 days. The safety of the study drug and its efficacy in infantile colic symptoms were assessed after the end of the treatment. Results: Among 200 patients, 4 (2%) adverse events (AEs) were reported. They were mild, not related to the study drug, and resolved without sequelae. The mean crying time was reduced from 3.35±1.68 hours/day at baseline to 0.37±0.67 hours/day on day 7 (mean reduction: -2.98; 95%CI: -3.24 to -2.72, p<0.001). The mean number of daily episodes of colic reduced from 3.09±1.90 at baseline to 0.47±0.88 on day 7 (mean difference: -2.61; 95%CI: -2.90 to -2.33; p<0.001). A statistically significant (p<0.001) reduction was observed in excessive crying, fussing, sleep disturbances, clenching of fists, bending of arms and legs towards the belly, bloated tummy, redness of the face, flatulence and milk regurgitation on Day 7 as compared to the baseline. Complete remission of infantile colic was reported in 67.84% of patients after 7 days of treatment. Conclusion: TumsUP reduced the duration and severity of infantile colic and showed good safety, efficacy and tolerability.
Keywords: Infantile colic, Simethicone, Dill oil, Fennel oil, Fixed-dose combination
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , MBBS, MD (Pharmacology), Director, Department of Medical Services, Zuventus Healthcare Limited, Mumbai, Maharashtra, India. Email:  |
Bhupesh Dewan, Siddheshwar Shinde, TumsUP Drops: Evaluation of safety and efficacy in infantile colic.. Pediatric Rev Int J Pediatr Res. 2023;10(1):10-17. Available From https://pediatrics.medresearch.in/index.php/ijpr/article/view/735 |
 |
 ©
©  Figure 1: Disposition of subjects
Figure 1: Disposition of subjects
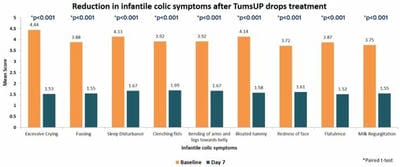 Figure 4: Reduction in infantile colic symptoms
Figure 4: Reduction in infantile colic symptoms