Common Tropical fevers: Experience from a tertiary care teaching hospital in North India
Chandra S.1*, Garg H.2, Rai N.3, Malik R.4, Nain T.5, Gupta M.6
DOI: https://doi.org/10.17511/ijpr.2023.i03.02
1* Surabhi Chandra, Professor& Head of Department, Department of Pediatrics, SRMS-IMS, Bhojipura, Bareilly, Uttar Pradesh, India.
2 Himanshu Garg, Post graduate Residents, Department of Pediatrics, SRMS-IMS, Bhojipura, Bareilly, Uttar Pradesh, India.
3 Namrata Rai, Post graduate Residents, Department of Pediatrics, SRMS-IMS, Bhojipura, Bareilly, Uttar Pradesh, India.
4 Ritu Malik, Post graduate Residents, Department of Pediatrics, SRMS-IMS, Bhojipura, Bareilly, Uttar Pradesh, India.
5 Tanveer Nain, Post graduate Residents, Department of Pediatrics, SRMS-IMS, Bhojipura, Bareilly, Uttar Pradesh, India.
6 Mayank Gupta, Post graduate Residents, Department of Pediatrics, SRMS-IMS, Bhojipura, Bareilly, Uttar Pradesh, India.
Background:We aimed at studying the clinical-laboratory profile of tropical fever, presenting to a tertiary care hospital.Materials and methods: The study was done after obtaining ethical clearance. In this prospective observational study, done from January 2022 to December 2022, patients fulfilling clinical criteria and confirmed positive on laboratory investigations were enrolled. They were managed and followed up during the hospital stay. Details were recorded, after obtaining written informed consent from parents.Results: A total of 118 patients who fulfilled the inclusion criteria were finally enrolled for analysis. The mean age of presentation was 12.9 years (Range 8-16 years; SD 2.169). The majority of cases, especially those known to be transmitted by mosquitoes, were seen in the post-monsoon season (50/118 = 42.3%). Typhoid or enteric fever (39/118 = 33.0%) was the major etiology. There was an overlap in clinical findings with hepatosplenomegaly being the most common one seen in 94.0% of cases and the least common finding was lymphadenopathy (5.5%) cases. A third (36/118 = 30.5%) of these patients required PICU admission sometime during hospitalization.Of the patients who required admission to PICU, around 90% required inotropic/ vasoactive support, 72.8% (59% non-invasive and 13.8% invasive) required ventilator support and 14.6% patients required renal replacement therapy. One hundred and eleven (111/118 = 94.0%) patients survived and recovered completely.Conclusion: Enteric fever was the most common etiology of Tropical Fever in this study. The majority of cases of tropical fever had intact survival and did not require PICU admission.
Keywords: Tropical Fever, Enteric Fever, Clinico-Laboratory Profile
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Professor& Head of Department, Department of Pediatrics, SRMS-IMS, Bhojipura, Bareilly, Uttar Pradesh, India. Email:  |
Surabhi Chandra, Himanshu Garg, Namrata Rai, Ritu Malik, Tanveer Nain, Mayank Gupta, Common Tropical fevers: Experience from a tertiary care teaching hospital in North India. Pediatric Rev Int J Pediatr Res. 2023;10(3):41-45. Available From https://pediatrics.medresearch.in/index.php/ijpr/article/view/749 |
 |
 ©
© 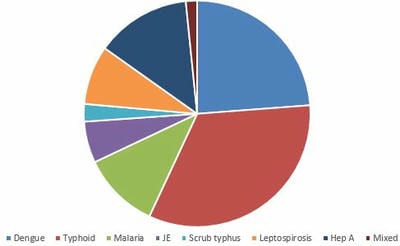 Figure 1:Etiological Profile of Tropical Fever
Figure 1:Etiological Profile of Tropical Fever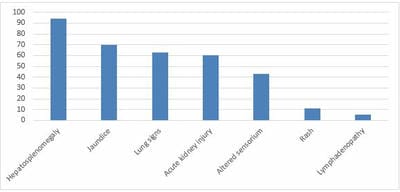 Figure 2.Clinical Findings in Patients with Tropical Fever
Figure 2.Clinical Findings in Patients with Tropical Fever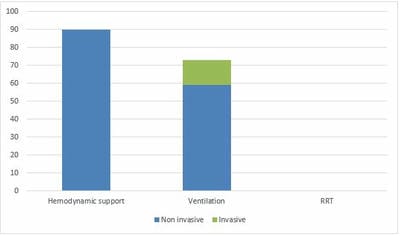 Figure 3. Critical care support required
Figure 3. Critical care support required