A Rare Occurrence of Total Anomalous Pulmonary Venous Return in Dichorionic Diamniotic Twins
Badugu V.1, Venkata Rama Susarla B.2*, Kumar Chintapally S.3, Kulkarni Bhaskar Rao A.4, Gattu H.5, Dignesh Kumar B.6
DOI: https://doi.org/10.17511/ijpr.2023.i03.06
1 Venkatesh Badugu, Consultant, Department of Neonatology, Ankura hospital for Women and Children, Boduppal, Hyderabad, Telengana, India.
2* Balaji Venkata Rama Susarla, Consultant, Department of Neonatology, Ankura hospital for Women and Children, Boduppal, Hyderabad, Telengana, India.
3 Suman Kumar Chintapally, Consultant, Department of Neonatology, Ankura hospital for Women and Children, Boduppal, Hyderabad, Telengana, India.
4 Ajay Kulkarni Bhaskar Rao, Consultant, Department of Neonatology, Ankura hospital for Women and Children, Boduppal, Hyderabad, Telengana, India.
5 Harshitha Gattu, Consultant, Department of Neonatology, Ankura hospital for Women and Children, Boduppal, Hyderabad, Telengana, India.
6 Barala Dignesh Kumar, Consultant, Department of Neonatology, Ankura hospital for Women and Children, Boduppal, Hyderabad, Telengana, India.
Congenital heart defects (CHDs) represent the most common human birth defect, having a birth prevalence of 7-9 per 1000 singleton births. CHDs are more common in twin pregnancies with a prevalence of approximately 20 in 1000 live births. Monochorionic (MC) twins are at even higher risk compared to Dichorionic (DC) twins. Herein, we report a scenario where Dichorionic Diamniotic (DCDA) twins presented with the same type of CHD (TAPVR: Total anomalous pulmonary venous return) in our Neonatal intensive care unit(NICU). Several familial cases of TAPVR have been reported, but no notable pedigree has been reported. Multiple case reports have shown a genetic background of TAPVR. Screening of all siblings with TAPVR is a burden to the patients due to psychological stress or financial problems for the parents. However, these consequences are outweighed by the benefit of diagnosing this critical disease early so that the patient can be taken for surgery before severe congestive heart failure develops. Therefore, if a genetic background is detected in a case of TAPVR, routine fetal echocardiography or cardiography immediately after birth is reasonable to screen TAPVR.
Keywords: Congenital Heart Defects, Total Anomalous Pulmonary Venous Return, Twins
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Consultant, Department of Neonatology, Ankura hospital for Women and Children, Boduppal, Hyderabad, Telengana, India. Email:  |
Venkatesh Badugu, Balaji Venkata Rama Susarla, Suman Kumar Chintapally, Ajay Kulkarni Bhaskar Rao, Harshitha Gattu, Barala Dignesh Kumar, A Rare Occurrence of Total Anomalous Pulmonary Venous Return in Dichorionic Diamniotic Twins. Pediatric Rev Int J Pediatr Res. 2023;10(3):65-68. Available From https://pediatrics.medresearch.in/index.php/ijpr/article/view/752 |
 |
 ©
©  Figure 1: Chest x-ray of twin 1 depicting ground glass opacities and reticulogranular
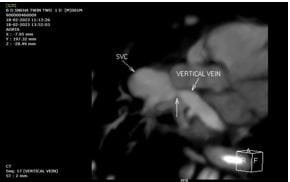
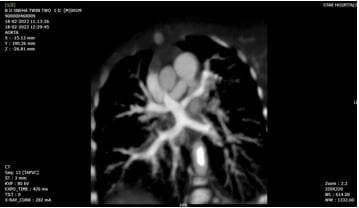
Figure 1: Chest x-ray of twin 1 depicting ground glass opacities and reticulogranular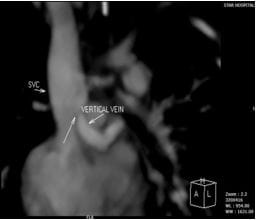 Figure 2: Note the CT angiography image of twin 1 showing the pulmonary veins draining into the superior vena cava(SVC) via the vertical vein revealing the supracardiac variety of TAPVR.
Figure 2: Note the CT angiography image of twin 1 showing the pulmonary veins draining into the superior vena cava(SVC) via the vertical vein revealing the supracardiac variety of TAPVR.