Association of Neural Tube Defects of Newborn with Maternal Serum Vitamin-B12 level-A Review Study
Badal F1*, Rashid F2, Pervin R3, Naher N4, Khanam M5
DOI:https://doi.org/10.17511/ijpr.2024.i02.01
1* FA Badal, Assistant Professor, Department of Neonatology, Shaheed Ziaur Rahman Medical College, Bogura, Bogra, Bangladesh.
2 FJB Rashid, Assistant Surgeon, Obstetrics and Gynecology, Sheikh Hasina Medical College Hospital, Tangail, Bangladesh.
3 R Pervin, Assistant Professor, Obstetrics and Gynecology, Sheikh Hasina Medical College, Tangail, Bangladesh.
4 N Naher, Junior Consultant, Gynae and Obs, Bedded General Hospital, Tangail, Bangladesh.
5 M Khanam, Junior Consultant, Gynae and Obs, Sheikh Hasina Medical College Hospital, Tangail, Bangladesh.
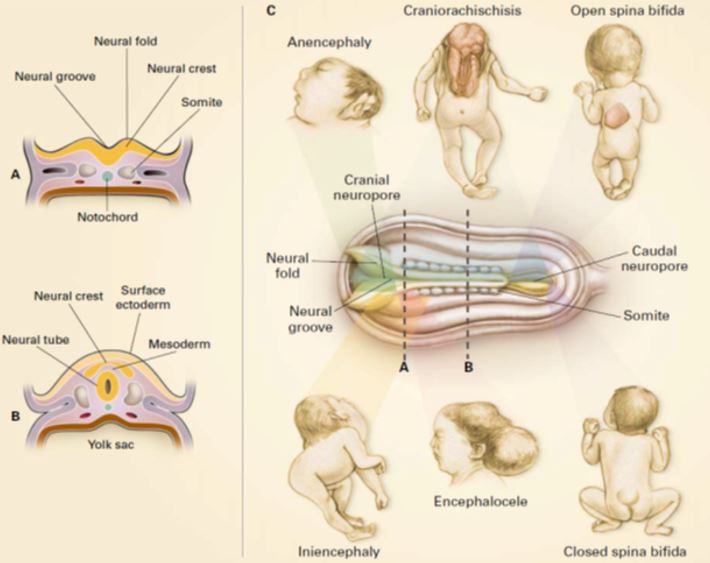
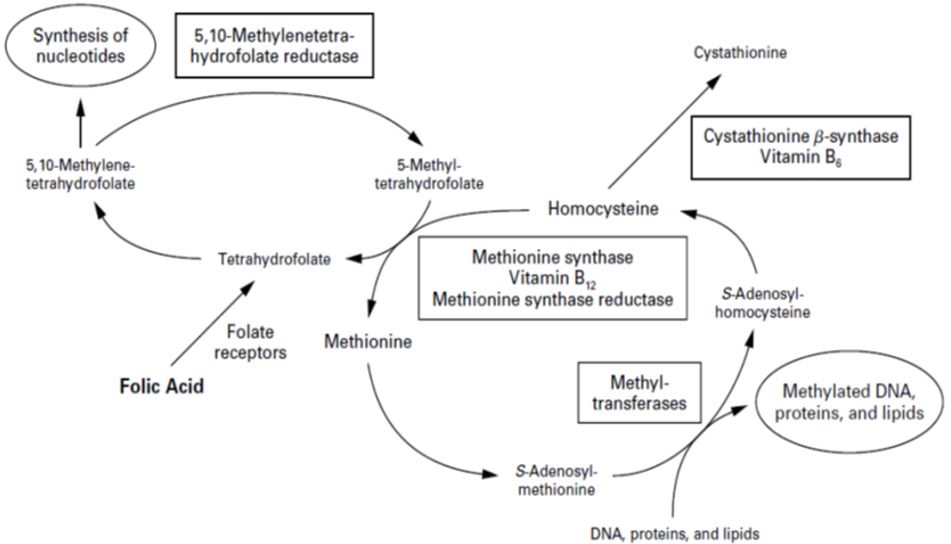
Neural tube defects (NTDs) are one of the most common birth defects in our clinical practices. Maternal nutritional factors are associated with an increased chance of development of NTDs in offspring. Periconceptional folic acid supplementation can prevent up to three-fourths of neural tube defects (NTDs). Some studies reported that there might be an association between maternal serum vitamin B12 levels and NTDs. Dietary vitamin B12 deficiency is a common problem in the Indian subcontinent including Bangladesh because of inadequate dietary intake, dietary habits and/or malabsorption. There is a scarcity of studies to establish the relationship between vitamin B12 and NTDs. It would be beneficial to see the association of vitamin B12 and NTDs in a Bangladeshi population, which may help in deciding about vitamin B12 supplementation as a preventive measure of NTDs.
Keywords: NTDs, Maternal and Neonatal Serum, vitamin B12 level
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Assistant Professor, Department of Neonatology, Shaheed Ziaur Rahman Medical College, Bogura, Bogra, Bangladesh. Email:  |
Badal F, Rashid F, Pervin R, Naher N, Khanam M, Association of Neural Tube Defects of Newborn with Maternal Serum Vitamin-B12 level-A Review Study. Pediatric Rev Int J Pediatr Res. 2024;11(2):7-14. Available From https://pediatrics.medresearch.in/index.php/ijpr/article/view/765 |
 |
 ©
©