Factors Hindering Compliance with Exclusive Breastfeeding Practices Among Mothers: A Narrative Review
Kadiyan P1*, Verma M2, Shafqat N3, Anjali A, Vada S4
DOI:https://doi.org/10.17511/ijpr.2024.i03.06
1* Priya Kadiyan, Msc Nursing Student, Nursing, All India Institute of Medical Sciences, Bhopal, Madhya Pradesh, India.
2 Mamta Verma, Associate Professor, Nursing, All India Institute of Medical Sciences, Bhopal, Madhya Pradesh, India.
3 Naseema Shafqat, Assistant Professor, Nursing, All India Institute of Medical Sciences, Bhopal, Madhya Pradesh, India.
4 Akanksha Anjali, MSc Nursing Student, Nursing, All India Institute of Medical Sciences, Bhopal, Madhya Pradesh, India.
5 Satyam Vada, MSc Nursing Student, Nursing, All India Institute of Medical Sciences, Bhopal, Madhya Pradesh, India.
Introduction: Commencing a child's developmental path with the unparalleled advantages of exclusive breastfeeding establishes the cornerstone for optimal health. Despite understanding the importance of exclusive breastfeeding (EBF), many mothers still face challenges in adhering to it. The objective of this review is to thoroughly delineate the barriers to exclusive breastfeeding.
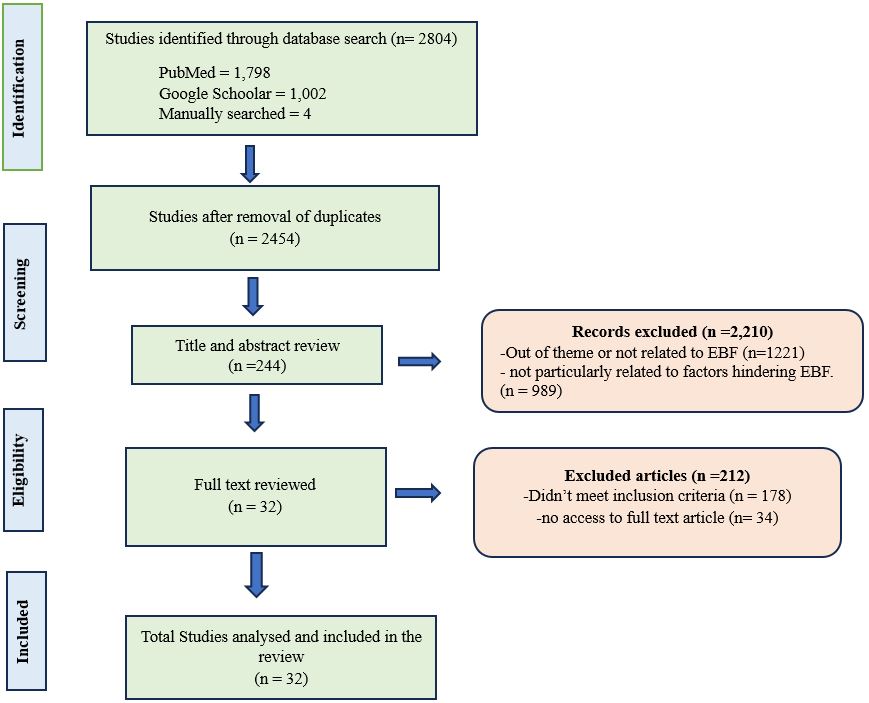
Methods: Searches were conducted using PubMed, Google Scholar, and manually to retrieve studies from 2014-2024. Using our inclusion criteria, we selected studies that described barriers to exclusive breastfeeding. Qualitative and quantitative studies and survey reports published in English were considered. The descriptors used in this study were: factors, determinants, causes, barriers, hindering, influencing, and exclusive breastfeeding. Thirty-two studies from various countries were included.
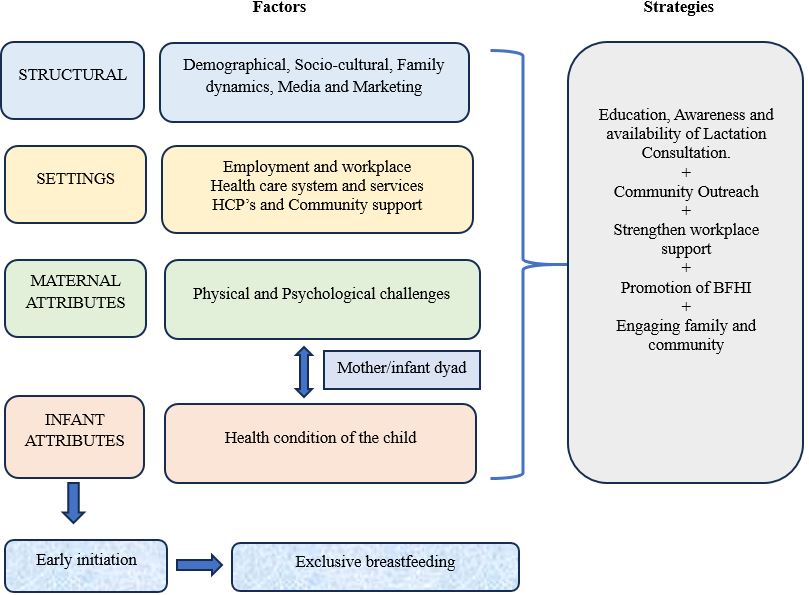
Result: Out of the 244 articles identified, 32 met the inclusion criteria. Most of the included studies were cross-sectional and were published between 2014 and 2024. Evidence indicates that breastfeeding support is crucial for extending both the duration and exclusivity of breastfeeding. Factors such as physiological issues, health-related barriers, and limitations within the healthcare system significantly impact exclusive breastfeeding practices. Interventions addressing these factors are essential for improving exclusive breastfeeding rates and enhancing maternal and child health outcomes.
Conclusion: Despite being widely practised, exclusive breastfeeding (EBF) rates remain low due to challenges faced by many mothers. Addressing these barriers through targeted interventions during antenatal and postnatal education can help improve and sustain EBF practices.
Keywords: factors, determinants, causes, barriers, hindering, influencing, exclusive breastfeeding
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Msc Nursing Student, Nursing, All India Institute of Medical Sciences, Bhopal, Madhya Pradesh, India. Email:  |
Kadiyan P, Verma M, Shafqat N, Anjali A, Vada S, Factors Hindering Compliance with Exclusive Breastfeeding Practices Among Mothers: A Narrative Review. Pediatric Rev Int J Pediatr Res. 2024;11(3):49-57. Available From https://pediatrics.medresearch.in/index.php/ijpr/article/view/773 |
 |
 ©
©