Early Initiation of Breastfeeding: Caesarean Mothers’ Challenges and Coping
Khan MM1*, Verma M2, Gupta R3
DOI:https://doi.org/10.17511/ijpr .2025.i02.03
1* Mussarat Musera Khan, MSc Nursing Student, Pediatric Nursing, Nursing College, All India Institute of Medical Sciences, Bhopal, India.
2 Mamta Verma, PhD, Faculty of Pediatric Nursing, Nursing College, All India Institute of Medical Sciences, Bhopal, India.
3 Rajratan Gupta, Faculty of Nursing, Nursing College, All India Institute of Medical Sciences, Bhopal, India.
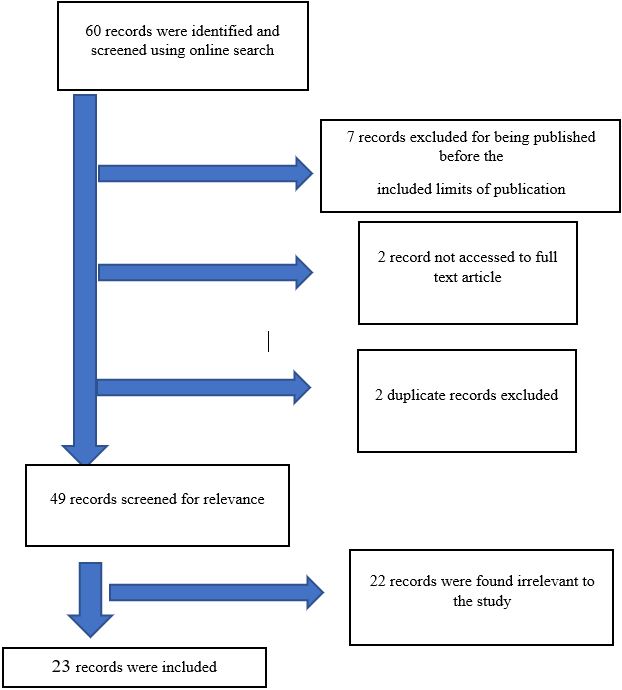
This narrative review aims to identify the available literature related to factors related to caesarean section and early initiation of breastfeeding, challenges which cause hindrance to early initiation of breastfeeding and the coping strategies mothers could employ to overcome the challenges. The narrative review secondarily helps the author to select the study design, methodology and development of the questionnaire. It is a well-known fact that early initiation of breastfeeding is an essential component in the crucial first hour after birth. The review compares the data obtained through various searches regarding early initiation of breastfeeding in vaginal and caesarean delivery. Also, some factors which are responsible for delay especially in the case of caesarean section are identified which would help in the planning of assessment questionnaire components. Apart from caesarean section delivery being the main determinant for late initiation of breastfeeding, the associated clues like post-operative pain, delayed mother-newborn dyad contact, and lack of maternal efficiency in handling newborns after birth play an important role in determining breastfeeding initiation. Family and partner support had a great role in coping with post-partum anxiety.
Keywords: early initiation of breastfeeding (EIBF), caesarean section, vaginal delivery, challenges, coping strategies
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , MSc Nursing Student, Pediatric Nursing, Nursing College, All India Institute of Medical Sciences, Bhopal, , India. Email:  |
Khan MM, Verma M, Gupta R, Early Initiation of Breastfeeding: Caesarean Mothers’ Challenges and Coping. Pediatric Rev Int J Pediatr Res. 2025;12(2):31-40. Available From https://pediatrics.medresearch.in/index.php/ijpr/article/view/790 |
 |
 ©
©