Goldenhar syndrome: rare case reported from secondary health care facility in Himachal Pradesh
Dharmani A.1, Sharma V.2, Thakur S.3, Kashyap S.4
DOI: https://doi.org/10.17511/ijpr.2020.i01.08
1 Ankur Dharmani, MD Pediatrics, (PGIMER Chandigarh), Regional Hospital, Bilaspur, Himachal Pradesh, India.
2 Vandna Sharma, MS Ophthalmology (Dr RPGMC TANDA), Regional Hospital, Bilaspur, Himachal Pradesh, India.
3 Swati Thakur, MD Radiodiagnosis (AIIMS New Delhi), Phoenix Diagnostic Center, Bilaspur, Himachal Pradesh, India.
4 Sonia Kashyap, MD Internal Medicine (PGIMER Chandigarh), DDU Hospital, Shimla, Himachal Pradesh, India.
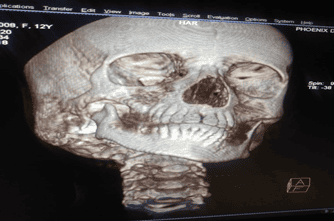
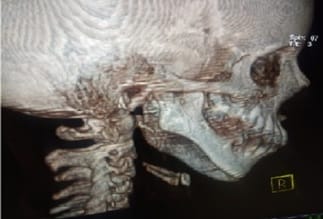
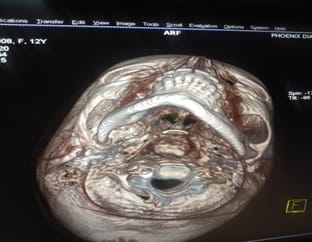
Dr. Maurice Goldenhar, a renowned Swiss ophthalmologist classified the clinical features and named the malformation complex as Goldenhar Syndrome and described it as a congenital defect characterized by constellation of malformations classically involving the face, eyes and ears. Principal deformities of the Goldenhar syndrome are often combined with various malformations, like Cleft lip and/or palate, tongue cleft, unilateral tongue hypoplasia, and parotid gland aplasia, Rib anomalies, Congenital heart disease (ventricular septal defects). A 12-year-old female patient diagnosed with Goldenhar syndrome at secondary care Regional Hospital Bilaspur, Himachal Pradesh. She was diagnosed with a case of Goldenhar syndrome on clinic-radiological investigations. The patient reported to ophthalmology OPD of the hospital with the chief complaint of soft tissue structure in left eye with decreased vision. On examination limbal dermoid was observed. Patient was having pre-auricular tissue tag on both sides, hemifacial micrognathia and microstomia. Correlating the history and physical findings a provisional diagnosis of Goldenhar Syndrome was made with differential diagnosis of Franschetti syndrome or Treacher – Collins syndrome, Nager syndrome or acro-facial dysostosis and Townes-Brocks syndrome. Based on the clinical and radiographic findings a diagnosis of Goldenhar syndrome was made. Severe cases of GS can affect the routine and social life of the patient. Early detection can help avoid complications at a later stage of life. Such patients will have an increased risk for psychosocial difficulties. The study of this condition is still controversial because the symptoms and the physical features may vary greatly in range and severity from case to case.
Keywords: Goldenhar syndrome, Oculo-auriculo-vertebral (OAV) dysplasia, Congenital defects
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Internal Medicine (PGIMER Chandigarh), DDU Hospital, Shimla, Himachal Pradesh, India. Email: dr.sonia21@gmail.com |
Dharmani A, Sharma V, Thakur S, Kashyap S. Goldenhar syndrome: rare case reported from secondary health care facility in Himachal Pradesh. Pediatric Rev Int J Pediatr Res. 2020;7(1):42-48. Available From https://pediatrics.medresearch.in/index.php/ijpr/article/view/567 |
 |
 ©
©