Assessment of prevalence of risk factors for non-communicable diseases in early adolescent age group using Global School Health Survey in Ujjain, Madhya Pradesh, India
Sharma P.1, Chandra Mandliya J.2*, Dhaneria M.3, Diwan V.4
DOI: https://doi.org/10.17511/ijpr.2020.i06.02
1 Priyanka Sharma, Resident, Department of Pediatrics, R.D Gardi Medical College, Ujjain, Madhya Pradesh, India.
2* Jagdish Chandra Mandliya, Professor, Department of Pediatrics, R.D Gardi Medical College, Ujjain, Madhya Pradesh, India.
3 Mamta Dhaneria, Professor and Head, Department of Pediatrics, R.D Gardi Medical College, Ujjain, Madhya Pradesh, India.
4 Vishal Diwan, Scientist E, National Institute for Research in Environmental Health, Bhopal, Madhya Pradesh, India.
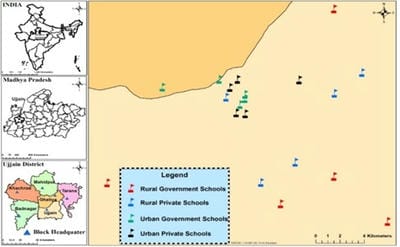
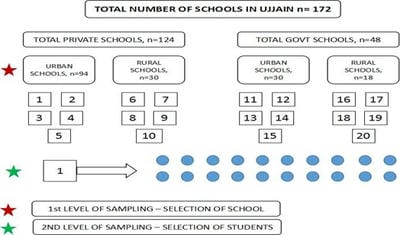
Introduction: There has been a global rise in non-communicable diseases and a shift in trends from infectious to chronic lifestyle-related diseases, roots of which are behaviourally acquired and begin during adolescence. Adolescence constitutes a natural partner for their prevention. Objective: To determine the prevalence of risk factors for non-communicable diseases in the early adolescent age group using a global school-based health survey among students of Ujjain. Method: Cross-sectional study was done for 24 months from August 2017 to August 2019 in schools of Ujjain, Madhya Pradesh. Sampling was done using a cluster sampling technique. Students who participated were administered a questionnaire based on the GLOBAL SCHOOL HEALTH SURVEY. Appropriate statistical methods were used to find the odds ratio for the prevalence of the risk factors and differences among sex, residence (urban or rural), and type of school (government or private). Result: This study documents that among 400 students lack exercise, consumption of junk food =44.5%, high alcohol consumption 16.8 %, smoking cigarettes was found to be prevalent risk factors of NCDs. There was a statistically significant difference noted among types of school, residence, and sex. Conclusion: This is the first study done in this region and emphasizes individual health interventions along with the implementation of national health policies targeting the adolescent age group to lower the financial and health care burden of the region.
Keywords: Non-communicable Diseases (NCD), WHO, Age
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Professor, Department of Pediatrics, R.D Gardi Medical College, Ujjain, Madhya Pradesh, India. Email:  |
Sharma P, Mandliya JC, Dhaneria M, Diwan V. Assessment of prevalence of risk factors for non-communicable diseases in early adolescent age group using Global School Health Survey in Ujjain, Madhya Pradesh, India. Pediatric Rev Int J Pediatr Res. 2020;7(6):228-236. Available From https://pediatrics.medresearch.in/index.php/ijpr/article/view/609 |
 |
 ©
©