To study the correlation between various levels of cord blood albumin & serum bilirubin at 48 hrs of age in term healthy newborns
Arya S.1, Panwar C.2, Prajapati J.3*
DOI: https://doi.org/10.17511/ijpr.2021.i03.04
1 Sunil Arya, Associate professor, Department of Pediatrics, MGM Medical College, Indore, Madhya Pradesh, India.
2 Chetan Panwar, Senior resident, Department of Pediatrics, MGM Medical College, Indore, Madhya Pradesh, India.
3* Jyoti Prajapati, Assistant professor, Department of Pediatrics, MGM Medical College, Indore, Madhya Pradesh, India.
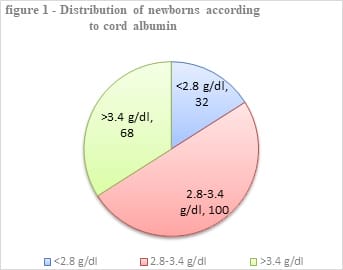
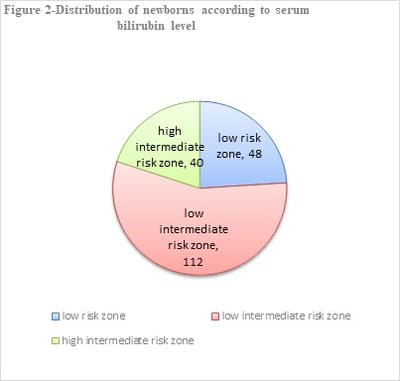
Introduction: Neonatal Hyperbilirubinemia is the most common abnormal physical finding and the major cause of neonatal morbidity during the early neonatal period. Early identification of infants at risk might help in providing preventative therapy and follow-up. We aimed to assess whether arterial umbilical cord albumin level at birth predicts the development of neonatal hyperbilirubinemia in term newborns at 48 hrs of life. Methods: This prospective observational cohort study was conducted in a tertiary care hospital over 1 year in 200 term healthy neonates. Cord blood albumin was estimated at birth followed by serum bilirubin level on the 3rd postnatal day(48 hrs of age). Results: Total of 200 neonates were divided into three groups based on cord blood albumin level of <2.8 g/dl(group I), 2.8-3.4 g/dl(group II) and >3.4 g/dl(groupIII) with 32, 100 and 68 in three respective groups. 19 newborns (59.4%) in group I,14 in group II, and 7 newborns (10.3%) in group III developed serum bilirubin levels above an intermediate high-risk zone in Bhutani nomogram at 48 hrs of age. newborn with low cord albumin (<2.8g/dl) were significantly associated with higher bilirubin levels at 48 hrs of age. Conclusion: Neonates with cord blood albumin <2.8 gm/dl had a significant association of the development of hyperbilirubinemia at or above intermediate high-risk zone according to Bhutani nomogram at 48 hrs of life.
Keywords: Neonatal hyperbilirubinemia, Cord blood albumin, Pathological hyperbilirubinemia, Serum bilirubin.
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Assistant professor, Department of Pediatrics, MGM Medical College, Indore, Madhya Pradesh, India. Email:  |
Arya S, Panwar C, Prajapati J. To study the correlation between various levels of cord blood albumin & serum bilirubin at 48 hrs of age in term healthy newborns. Pediatric Rev Int J Pediatr Res. 2021;8(3):146-151. Available From https://pediatrics.medresearch.in/index.php/ijpr/article/view/659 |
 |
 ©
©