4 Dimensional XStrain echocardiographic assessment by sequential chamber analysis of Double Outlet Left Ventricular with Tricuspid Atresia
Mehrotra A.1*, Singh S.2, Kacker S.3
DOI: https://doi.org/10.17511/ijpr.2022.i04.01
1* Akhil Mehrotra, Chief, Non-Invasive Cardiologist, Pediatric and Adult Cardiology, Prakash Heart Station, D-16, Nirala Nagar, Lucknow, U.P, India.
2 Swati Singh, Senior Echocardiography Technician, Pediatric and Adult Cardiology, Prakash Heart Station, D-16, Nirala Nagar, Lucknow, U.P, India.
3 Shubham Kacker, Senior coordinator, Project Management Office, Tech Mahindra, Noida, U.P, India.
Double outlet left ventricle (DOLV) is an extremely rare cyanotic congenital cardiac malformation with an incidence of less than 1 in 200,000 live births and usually manifests during the neonatal period. DOLV occurs most commonly in the form of atrial situs solitus with atrioventricular (AV) concordance but is often associated with myriads of cardiac anomalies such as VSD, ASD, PDA, pulmonary stenosis, right ventricular hypoplasia, and tricuspid atresia (TA). The clinical manifestations depend largely on the type of the associated cardiac defects, e.g. pulmonary or aortic outflow tract obstruction, resulting from pulmonary or aortic valve stenosis respectively. We are presenting an exceedingly rare case report of DOLV, tricuspid atresia, D-malposition of great arteries, and mild pulmonary stenosis with the absence of RV hypoplasia, assessed by sequential chamber analysis, employing 4Dimensional XStrain colour Doppler echocardiography.
Keywords: Double outlet left ventricle with tricuspid atresia, tricuspid atresia, D-malposition of great arteries, Atrial Septal Defect, Ventricular septal Defect, conus
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Chief, Non-Invasive Cardiologist, Pediatric and Adult Cardiology, Prakash Heart Station, D-16, Nirala Nagar, Lucknow, U.P, India. Email:  |
Akhil Mehrotra, Swati Singh, Shubham Kacker, 4 Dimensional XStrain echocardiographic assessment by sequential chamber analysis of Double Outlet Left Ventricular with Tricuspid Atresia. Pediatric Rev Int J Pediatr Res. 2022;9(4):14-20. Available From https://pediatrics.medresearch.in/index.php/ijpr/article/view/724 |
 |
 ©
©  Figure 1: X-ray chest PA: cardiomegaly, reduced pulmonary blood flow.
Figure 1: X-ray chest PA: cardiomegaly, reduced pulmonary blood flow. Figure 2: Twelve lead ECG: Left axis deviation, LVH.
Figure 2: Twelve lead ECG: Left axis deviation, LVH.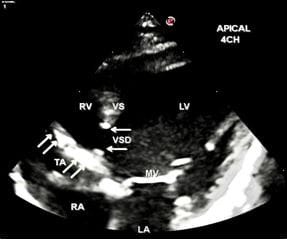 Figure 3: Apical 4CH view-Tricuspid atresia, large subaortic VSD, dilated LV, normal-sized RV. Horizontal arrows denote the presence of VSD, Oblique arrows denote Tricuspid atresia (TA).
Figure 3: Apical 4CH view-Tricuspid atresia, large subaortic VSD, dilated LV, normal-sized RV. Horizontal arrows denote the presence of VSD, Oblique arrows denote Tricuspid atresia (TA).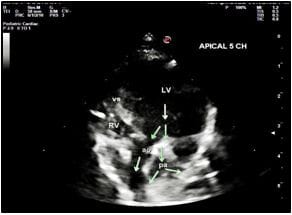 Figure 4: Apical 5CH view Double outlet left ventricle, D-malposition of great arteries, dilated LV ao, denotes Aorta pa, denotes Pulmonary Arteries.
Figure 4: Apical 5CH view Double outlet left ventricle, D-malposition of great arteries, dilated LV ao, denotes Aorta pa, denotes Pulmonary Arteries.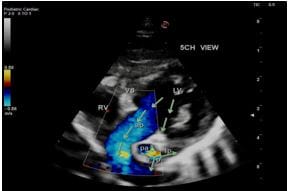 Figure 5: Apical 5CH view Double outlet left ventricle, Aorta is anterior and Pulmonary Artery is posterior, dilated LV, normal sized RV, hypoplasia of main and branch pulmonary arteries.
Figure 5: Apical 5CH view Double outlet left ventricle, Aorta is anterior and Pulmonary Artery is posterior, dilated LV, normal sized RV, hypoplasia of main and branch pulmonary arteries.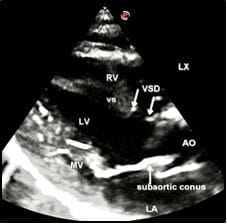 Figure 6: LAX view Subaortic VSD (moderate), characteristic subaortic conus, dilated LV.
Figure 6: LAX view Subaortic VSD (moderate), characteristic subaortic conus, dilated LV.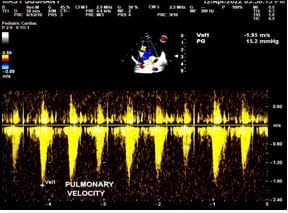 Figure 7: CW Doppler of the pulmonary artery:
Figure 7: CW Doppler of the pulmonary artery: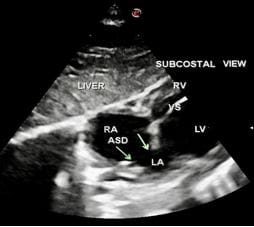 Figure 8: Subcostal View Large ostium secundum ASD denoted by oblique arrows.
Figure 8: Subcostal View Large ostium secundum ASD denoted by oblique arrows. Figure 9: LAX view Subaortic VSD (moderate size) denoted by arrows.
Figure 9: LAX view Subaortic VSD (moderate size) denoted by arrows.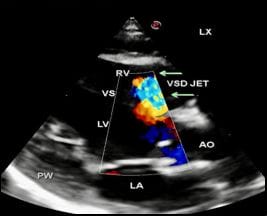 Figure 10: LAX view VSD jet is visualised with a left to right shunt across moderate size VSD.
Figure 10: LAX view VSD jet is visualised with a left to right shunt across moderate size VSD.