Double-Chambered Right Ventricle with Large Apical VSD- a Rare Case Report
Mehrotra A.1*, Sharma A.2, Singh S.3, Kacker S.4
DOI: https://doi.org/10.17511/ijpr.2022.i04.03
1* Akhil Mehrotra, Chief, Non-Invasive Cardiologist, Pediatric and Adult Cardiology, Prakash Heart Station, D-16, Nirala Nagar, Lucknow , U.P., India.
2 Ajay Sharma, Senior Echocardiography Technician, Pediatric and Adult Cardiology, Prakash Heart Station, D-16, Nirala Nagar, Lucknow , U.P., India.
3 Shwati Singh, Senior Echocardiography Technician, Pediatric and Adult Cardiology, Prakash Heart Station, D-16, Nirala Nagar, Lucknow , U.P., India.
4 Shubham Kacker, Senior Coordinator, Project Management Office, Tech Mahindra, Noida, U.P., India.
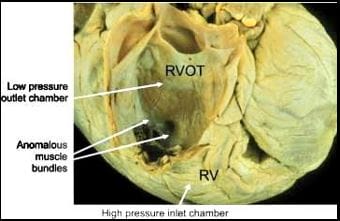
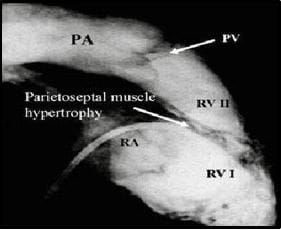
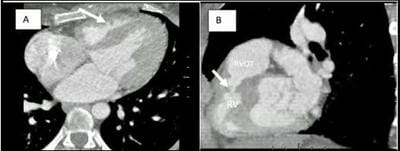
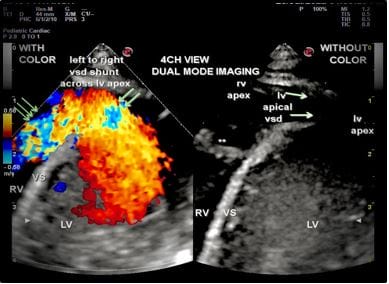
Double-chambered right ventricle (DCRV) is a rare condition seen in only 0.5 - 2.0% of all cases of congenital heart disease (CHD). An isolated DCRV is very rare, while approximately 80-90% of DCRV cases are associated with various other congenital heart defects, with VSD, in particular, a perimembranous type VSD, being the most common. In DCRV right ventricle is separated into a proximal high-pressure and distal low-pressure chamber. It can be caused either by the presence of an anomalous muscle bundle (AMB), by hypertrophy of endogenous trabecular tissue, or occasionally by an aberrant moderator band. DCRV is characterised by intraventricular pressure gradients greater than 20 mmHg, turbulent flow patterns in the ventricle, and increased pulmonary blood flow. Currently, the methods for detection of DCRV with VSD are Colour echocardiography, Cardiac catheterization, Cardiac CT and Cardiac MRI. This anomaly is often diagnosed during childhood and adolescence, while very few are found in adults. Here, we are presenting an extremely rare case report of a 7-month-old male child afflicted with symptomatic DCRV, unusually associated with a large apical muscular VSD.
Keywords: Double-chambered right ventricle, Large Apical VSD, 4Diemensional XStrain Echocardiography, Anomalous Muscle bundle
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Chief, Non-Invasive Cardiologist, Pediatric and Adult Cardiology, Prakash Heart Station, D-16, Nirala Nagar, Lucknow , U.P., India. Email:  |
Akhil Mehrotra, Ajay Sharma, Shwati Singh, Shubham Kacker, Double-Chambered Right Ventricle with Large Apical VSD- a Rare Case Report. Pediatric Rev Int J Pediatr Res. 2022;9(4):25-33. Available From https://pediatrics.medresearch.in/index.php/ijpr/article/view/726 |
 |
 ©
©