
Double-Chambered Right Ventricle with Large Apical VSD- a Rare Case Report
Abstract
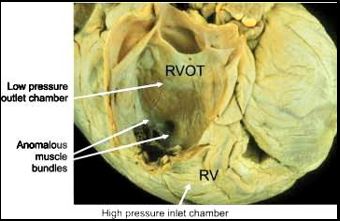
Double-chambered right ventricle (DCRV) is a rare condition seen in only 0.5 - 2.0% of all cases ofcongenital heart disease (CHD). An isolated DCRV is very rare, while approximately 80-90% ofDCRV cases are associated with various other congenital heart defects, with VSD, in particular, aperimembranous type VSD, being the most common. In DCRV right ventricle is separated into aproximal high-pressure and distal low-pressure chamber. It can be caused either by the presence ofan anomalous muscle bundle (AMB), by hypertrophy of endogenous trabecular tissue, oroccasionally by an aberrant moderator band. DCRV is characterised by intraventricular pressuregradients greater than 20 mmHg, turbulent flow patterns in the ventricle, and increased pulmonaryblood flow. Currently, the methods for detection of DCRV with VSD are Colour echocardiography,Cardiac catheterization, Cardiac CT and Cardiac MRI. This anomaly is often diagnosed duringchildhood and adolescence, while very few are found in adults. Here, we are presenting anextremely rare case report of a 7-month-old male child afflicted with symptomatic DCRV, unusuallyassociated with a large apical muscular VSD.
Downloads
References
[1] Nagashima M, Tomino T, Satoh H, Nakata T, Ohtani T, Saito H. Double-chambered right ventricle in adulthood. Asian Cardiovasc Thorac Ann 2005; 13:27-30.
[2] Hoffman P, Wojcik AW, Rozanski J, Siudalska H, Jakubowska E, Wlodarska EK, Kowalski M. The role of echocardiography in diagnosing double chambered right ventricle in adults. Heart 2004; 90:789-93.
[3] Restivo A, Cameron AH, Anderson RH, Allwork SP. Divided right ventricle: a review of its anatomical varieties. Pediatr Cardiol 1984; 5:197-204.
[4] Wang JK, Wu MH, Chang CI, Chiu IS, Chu SH, Hung CR, Lue HC. Malalignment-type ventricular septal defect in double-chambered right ventricle. Ann J Cardiol 1996; 77:839-42.
[5] Alva C, Ho SY, Lincoln CR, Rigby ML, Wright A, Anderson RH. The nature of the obstructive muscular bundles in double-chambered right ventricle. J Thorac Cardiovasc Surg 1999; 117: 1180-9.
[6] Brock RC. The anatomy of congenital pulmonary stenosis. London: Cassel; 1957.42-51.
[7] Keith A. The Hunterian lectures of malformations of the heart. Lancet 1909; 2:359.
[8] Lucas Jr RV, Varco RL, Lillehei CW, Adams Jr P, Anderson RC, Edwards JE. Anomalous muscle bundle of the right ventricle. Hemodynamic consequences and surgical considerations. Circulation 1962; 25:443-55.
[9] Tsifutis AA, Hartmann Jr AF, Arvidsson H. Two-chambered right ventricle: report on seven patients. Circulation 1961; 24:1058.
[10] Folger Jr GM. Right ventricular outflow pouch associated with double-chambered right ventricle. Am Heart J 1985; 109:1044-9.
[11] Park JG, Ryu HJ, Jung YS, Kim KJ, Lee BR, Jung BC, Kang H. Isolated double-chambered right ventricle in a young adult. Korean Circ J 2011; 41:272-5.
[12] Yuan SM. Congenital heart defects in Williams’s syndrome. Turk J Pediatr 2017; 59:225-232.
[13] Oliver JM, Garrido A, Gonzalez A, Benito F, Mateos M, Aroca A, et al. Rapid progression of midventricular obstruction in adults with double-chambered right ventricle. J Thorac Cardiovasc Surg 2003; 126:711-7.
[14] Park JI, Kim Yh, Lee K, Park HK, Park CB. Isolated double chambered right ventricle presenting in adulthood. Int J Cardiol 2002; 121:28-27.
[15] Lascano ME, Schaad MS, Moodie DX, Murphy (D). Difficulty in diagnosing double-chambered right ventricle in adults. Am J Cardiol 2001; 88:816-813.
[16] Matine D, van doesburg nh, Fouron JC, Guerin R, Davignon A Subxiphoid two-dimensional echocardiographic diagnosis of doubles-chambered right ventricle.circulation 1983;67:885-858.
[17] Hubail ZJ, Ramaciotti C. spatial relationship between the ventricular septal defect and the anomalous muscle bundle in a double-chambered right ventricle. Congenit Heart Dis 2007; 2:421-423
[18] Kilner PJ, Slevers B, Meyer GP, Ho SY. Double chambered right ventricle of sub-infundibular stenosis assessed by cardiovascular magnetic resonance. J Cardiovasc Magn Reson 1983; 4: 373; 379.
[19] Shirali GS, Smith EO, Geva T. Quantitation of echocardiographic predictors of outcome in infants with isolated ventricular septal defect. Am Heart J. 1995; 130:1228-1235.
[20] Khositseth A. Large apical muscular ventricular septal defect asymptomatic due to anomalous muscle bundles in the right ventricle Congenit Heart Dis. 2007; 2:70-73.
[21] Grittner f, Daehnert I, Gutberlet M, et al. Late diagnosis of a congenital apical ventricular septal defect with complete closure by right ventricular trabeculations. European heart Journal cardiovascular imaging 2014; 15:230.
Copyright (c) 2022 Author (s). Published by Siddharth Health Research and Social Welfare Society

This work is licensed under a Creative Commons Attribution 4.0 International License.

 OAI - Open Archives Initiative
OAI - Open Archives Initiative