Hydranencephaly – A rare case of a neglected child with enlarging head size
Patel S.1*, Sandeep B.2, Kiran B.3
DOI: https://doi.org/10.17511/ijpr.2022.i05.02
1* Shefali Patel, Assistant Professor, Department of Paediatrics, East Point College of Medical Sciences and Research Centre, Bangalore, Karnataka, India.
2 B Sandeep, Professor, Department of Paediatrics, East Point College of Medical Sciences and Research Centre, Bangalore, Karnataka, India.
3 B Kiran, HOD & Professor, Department of Paediatrics, East Point College of Medical Sciences and Research Centre, Bangalore, Karnataka, India.
Hydranencephaly is a rare congenital abnormality characterized by the absence and replacement of the cerebral hemisphere by cerebrospinal fluid. Here we report a rare case of a child who presented very late at 2 years of age with a massively enlarged head size with spasticity of all four limbs, suspected of hydrocephalous at first while on further work up diagnosed to have hydranencephaly. This report is aimed to make clinicians aware of a rare condition which can present very late even up to 2 years of age.
Keywords: Hydranencephaly, cerebrospinal fluid, hydrocephalous, spasticity
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Assistant Professor, Department of Paediatrics, East Point College of Medical Sciences and Research Centre, Bangalore, Karnataka, India. Email:  |
Shefali Patel, B Sandeep, B Kiran, Hydranencephaly – A rare case of a neglected child with enlarging head size. Pediatric Rev Int J Pediatr Res. 2022;9(5):34-37. Available From https://pediatrics.medresearch.in/index.php/ijpr/article/view/728 |
 |
 ©
©  Fig 1: A 2 year old female child with massively enlarged head size. Note the visibly enlarged veins over the frontal and parietal regions of the head.
Fig 1: A 2 year old female child with massively enlarged head size. Note the visibly enlarged veins over the frontal and parietal regions of the head.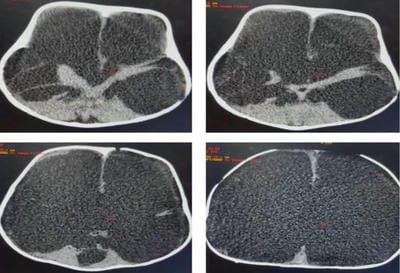 Figure 2: Axial non-contrast CT images of 2year old baby taken at multiple levels showing bilateral cerebral hemispheres being replaced by the fluid containing spaces of cerebrospinal fluid density. Normal posterior fossa, intact falx cerebri seen.
Figure 2: Axial non-contrast CT images of 2year old baby taken at multiple levels showing bilateral cerebral hemispheres being replaced by the fluid containing spaces of cerebrospinal fluid density. Normal posterior fossa, intact falx cerebri seen.