Prevalence, Pattern and Outcome of Blood Transfusion: A Private Paediatric Hospital Experience
A. West B.1*, Josephine E A.2
DOI: https://doi.org/10.17511/ijpr.2023.i01.01
1* Boma A. West, (FWACP), Department of Paediatrics and Child Health, Rivers State University Teaching Hospital, Nkpolu-Oroworukwo, Port Harcourt, Nigeria. 0000-0002-9849-1412
2 Aitafo Josephine E, (FWACP), Department of Paediatrics and Child Health, Rivers State University Teaching Hospital, Nkpolu-Oroworukwo, Port Harcourt, Nigeria. 0000-0003-3711-1495
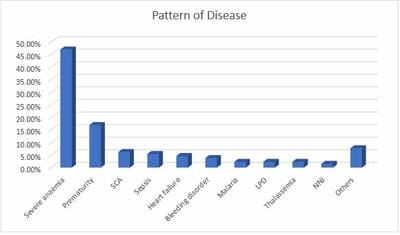
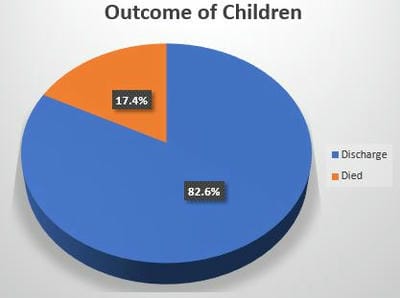
Introduction: Blood transfusion is an essential component of Pediatric care worldwide, especially in developing countries. Knowledge about its prevalence and pattern is vital in promoting its’ judicious use. Purpose: To ascertain the prevalence, pattern and outcome of blood transfusion in a private pediatric hospital in south-south Nigeria. Materials and Methods: A retrospective study was carried out over 1 year on children (0-17 years) admitted and transfused. Relevant data was retrieved from the hospitals’ Health Management System and analysed. Results: Of 1689 admissions, 69 were transfused giving a prevalence rate of 4.1% with male predominance (M: F ratio of 1.5:1). Eighty-eight blood transfusions were done giving a ratio of 1.3 transfusions/child. Transfused children were mainly 1–12 months of age with a mean age of 3.848 4.890 months. Most blood transfusions took place within the first 5 hours of prescription and occurred mostly at night. Sedimented cells were mainly used 49(71.0%). Nine(13.0%) children had blood transfusion reactions of which 5(60.0%) had a fever. The commonest diagnosis among children transfused were severe anaemia 61(46.9%), prematurity 22(16.9%), sickle cell anaemia 8(6.2%) and sepsis 7(5.4%). Twelve(17.4%) children transfused died. The age of children, the type of blood transfused and the number of transfusions carried out were significantly associated with the outcome of blood transfusion. Conclusion: The prevalence of blood transfusion was 4.1%. The commonest diagnosis was severe anaemia, prematurity, sickle cell anaemia and sepsis with a mortality rate of 17.4%. It is therefore important to equip private hospitals with functional blood bank services to reduce childhood morbidity and mortality.
Keywords: Blood transfusion, Outcome, Pattern, Prevalence
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , (FWACP), Department of Paediatrics and Child Health, Rivers State University Teaching Hospital, Nkpolu-Oroworukwo, Port Harcourt, Nigeria. Email:  |
Boma A. West, Aitafo Josephine E, Prevalence, Pattern and Outcome of Blood Transfusion: A Private Paediatric Hospital Experience. Pediatric Rev Int J Pediatr Res. 2023;10(1):1-9. Available From https://pediatrics.medresearch.in/index.php/ijpr/article/view/734 |
 |
 ©
©