A Rare Case Of Benzocaine-Induced Methemoglobinemia
Balaji S.1*, Suman Kumar C.2, Ravali G.3, Sravya P.4
DOI: https://doi.org/10.17511/ijpr.2023.i02.01
1* Susarla Balaji, Department of Neonatology, Ankura Hospital for Women and Children, Boduppal, Hyderabad, Telangana, India.
2 Chintapally Suman Kumar, Department of Neonatology, Ankura Hospital for Women and Children, Boduppal, Hyderabad, Telangana, India.
3 Gundapuneni Ravali, Department of Neonatology, Ankura Hospital for Women and Children, Boduppal, Hyderabad, Telangana, India.
4 Podishetti Sravya, Department of Neonatology, Ankura Hospital for Women and Children, Boduppal, Hyderabad, Telangana, India.
Methemoglobinemia is an uncommon haemoglobinopathy but potentially fatal if unrecognized or untreated at the earliest. It can either be congenital or acquired. Acquired can be after using topical anaesthetics such as nitrates, benzocaine, and lidocaine. The present study reports a rare case of benzocaine to induce Methaemoglobinemia. A 20-day-old male baby presented to the emergency room with complaints of seizure-like activity in the past hour, bluish discolouration of the skin for the past 1 day and loose watery stools for 3 days. The baby was irritable, crying with central cyanosis, and had 2 episodes of seizures upon arrival. He was tachypnoeic with saturations were 85% on room air along with tachycardia. Perianal rash with excoriation of overlying skin was present. The rest of the examination was unremarkable. He was managed with supplemental oxygen, IV antiepileptic and supportive treatment. His septic screen was normal; the Chest x-ray was unremarkable, and the 2D Echo showed a structurally normal heart with normal biventricular function. His percutaneous oxygen saturation remained 85-88% despite the administration of 100% oxygen. His arterial blood sample had a dark chocolate colour appearance, with normal PaO2 levels on blood gases. His methaemoglobin levels were 21.7%. After two doses of methylene blue (1 mg/kg/dose) were administered, his cyanosis abated and oxygenation improved. Repeat methaemoglobin levels were 1.3%. A relook into the history revealed the use of Mucopaine gel for a perianal rash which contains Benzocaine confirming it as Benzocaine-induced Methaemoglobinemia.
Keywords: Methaemoglobinemia, Benzocaine, Cyanosis
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , , Department of Neonatology, Ankura Hospital for Women and Children, Boduppal, Hyderabad, Telangana, India. Email:  |
Susarla Balaji, Chintapally Suman Kumar, Gundapuneni Ravali, Podishetti Sravya, A Rare Case Of Benzocaine-Induced Methemoglobinemia. Pediatric Rev Int J Pediatr Res. 2023;10(2):22-24. Available From https://pediatrics.medresearch.in/index.php/ijpr/article/view/740 |
 |
 ©
©  Figure 1: Note the central cyanosis over the lips, and tongue along with the mottled skin.
Figure 1: Note the central cyanosis over the lips, and tongue along with the mottled skin. 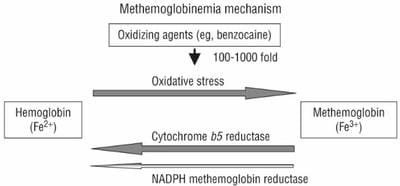 Figure 2: Mechanism ofMethaemoglobinemia
Figure 2: Mechanism ofMethaemoglobinemia