Modality of Respiratory Support in Preterm Neonates with Respiratory Distress and its Outcome: Experience of a Tertiary Care Hospital in Bangladesh
Abdul Mannan M.1*, Mandal S.2, Rasel M.3, Biswas B.4, Mahabub M.5, Rita F.6, Afroze S.7
DOI: https://doi.org/10.17511/ijpr.2023.i02.02
1* Md. Abdul Mannan, Professor, Department of Neonatology, Bangabandhu Sheikh Mujib Medical University (BSMMU), Dhaka, Bangladesh.
2 Shimul Mandal, Registrar, Department of Neonatology, Cumilla Medical College Hospital, Cumilla, Bangladesh.
3 Mohammad Rasel, Resident, Year-5, Department of Neonatology, Bangabandhu Sheikh Mujib Medical University (BSMMU), Dhaka, Bangladesh.
4 Baisakhi Biswas, Master in Public Health (Community Medicine), National Institute of Preventive and Social Medicine (NIPSOM), Dhaka, Bangladesh.
5 Maria Mahabub, Resident, Year-5, Department of Neonatology, Bangabandhu Sheikh Mujib Medical University (BSMMU), Dhaka, Bangladesh.
6 Farhana Rita, Resident, Year-4, Department of Neonatology, Bangabandhu Sheikh Mujib Medical University (BSMMU), Dhaka, Bangladesh.
7 Sharmin Afroze, Assistant Professor, Neonatology Unit, Dr. M R Khan Shishu Hospital & Institute of Child Health, Dhaka, Bangladesh.
Background: Preterm neonates are at increased risk of developing respiratory distress after birth. In order to reduce preterm death and their morbidity, identification of etiology and optimum management of respiratory distress is crucial. Objective: To determine causes of respiratory distress, pattern of respiratory modality used and its outcome among admitted preterm newborns. Material and methods: This study included 142 preterm neonates admitted with respiratory distress and required respiratory support in the NICU of Bangabandhu Sheikh Mujib Medical University, during the period from January 2020 to December 2021. Causes of respiratory distress and pattern of respiratory support was observed. Morbidities and in-hospital mortality were compared between invasive and non-invasive support group in the study. Results: Mean gestational age among the studied neonates was 32.39 ± 2.46 weeks. Male was predominant (54.2%) and mean birth weight was 1631.44 ± 578.57 g. About 62% belonged to the gestational age within 28 - <34 weeks category. Respiratory distress syndrome (RDS) was the most common cause which was 50.0% following TTN 24.6%, congenital pneumonia 19.0% and PNA 6.3%. Sepsis, septic shock, DIC, NEC and in-hospital mortality, nasal trauma, ROP and IVH occurred significantly higher in the mechanical ventilator support group in comparison to the NIV support group and the p-value were <0.05. Conclusion: In our study Respiratory distress syndrome is the commonest cause of respiratory distress. Invasive ventilation was associated with significant morbidity and mortality in preterm neonates when compared with those required non-invasive ventilation.
Keywords: Neonates, Preterm, Mechanical ventilation, Non-invasive ventilation
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Professor, Department of Neonatology, Bangabandhu Sheikh Mujib Medical University (BSMMU), Dhaka, , Bangladesh. Email:  |
Md. Abdul Mannan, Shimul Mandal, Mohammad Rasel, Baisakhi Biswas, Maria Mahabub, Farhana Rita, Sharmin Afroze, Modality of Respiratory Support in Preterm Neonates with Respiratory Distress and its Outcome: Experience of a Tertiary Care Hospital in Bangladesh. Pediatric Rev Int J Pediatr Res. 2023;10(2):25-31. Available From https://pediatrics.medresearch.in/index.php/ijpr/article/view/743 |
 |
 ©
© 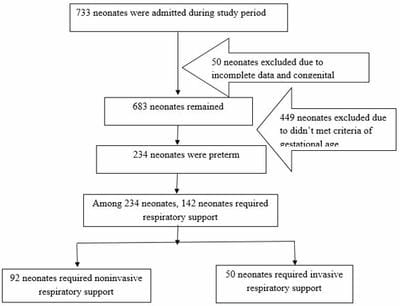 Figure 1: Flowchart of patient enrollment
Figure 1: Flowchart of patient enrollment