Childhood Hypertrophic Cardiomyopathy with Double Chambered Right Ventricle: A rare coexistence
Mehrotra A.1*, Shakya U.2, Kacker S.3
DOI: https://doi.org/10.17511/ijpr.2023.i03.04
1* Akhil Mehrotra, Chief, Non Invasive Cardiologist Pediatric and Adult Cardiology, Prakash Heart Station, D-16 Nirala Nagar, Lucknow, Uttar Pradesh, India.
2 Ujala Shakya, Cardiac Technician, Prakash Heart Station, D-16 Nirala Nagar, Lucknow, Uttar Pradesh, India.
3 Shubham Kacker, Lead PMO, Tech Mahindra, New Delhi, India.
The prevalence of hypertrophic cardiomyopathy (HCM) is about 0.05-0.2% of the general population. The occurrence of HCM is a significant cause of sudden cardiac death in any age group and a cause of heart failure. The generally accepted definition of HCM is a disease state characterised by unexplained left ventricular (LV) hypertrophy without dilatation of ventricular chambers in the absence of another cardiac or systemic disease, which itself is capable of producing the amplitude of hypertrophy, caused by a genetic disorder in one of the at least ten genes that encode the proteins of the cardiac sarcomere. The prevalence of double-chambered right ventricle (DCRV) with childhood HCM is unknown and extremely rare. We are presenting here a unique coexistence of HCM with severe left ventricular outflow (LVOT) obstruction and DCRV in a 5year old male child.
Keywords: Hypertrophic Cardiomyopathy, Double Chambered Right Ventricle, left ventricular outflow obstruction, SAM
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Chief, Non Invasive Cardiologist Pediatric and Adult Cardiology, Prakash Heart Station, D-16 Nirala Nagar, Lucknow, Uttar Pradesh, India. Email:  |
Akhil Mehrotra, Ujala Shakya, Shubham Kacker, Childhood Hypertrophic Cardiomyopathy with Double Chambered Right Ventricle: A rare coexistence. Pediatric Rev Int J Pediatr Res. 2023;10(3):51-56. Available From https://pediatrics.medresearch.in/index.php/ijpr/article/view/750 |
 |
 ©
©  Figure 1: Long-axis anatomy typical of hypertrophic cardiomyopathy. A: Anatomic specimen shows a tremendous increase in left ventricular wall thickness, but the increase in myocardial mass is most prominently displayed in the ventricular septum (asterisk). B: Echocardiographic image displays similar anatomy. The increase in myocardial thickness is less prominent than in the anatomic example, but the basal septum (yellow arrow) is still asymmetrically thickened relative to the posterior left ventricular wall. A anterior; Ao, aorta; LA, left atrium; LV, left ventricle; S, superior; VS, ventricular septum.
Figure 1: Long-axis anatomy typical of hypertrophic cardiomyopathy. A: Anatomic specimen shows a tremendous increase in left ventricular wall thickness, but the increase in myocardial mass is most prominently displayed in the ventricular septum (asterisk). B: Echocardiographic image displays similar anatomy. The increase in myocardial thickness is less prominent than in the anatomic example, but the basal septum (yellow arrow) is still asymmetrically thickened relative to the posterior left ventricular wall. A anterior; Ao, aorta; LA, left atrium; LV, left ventricle; S, superior; VS, ventricular septum. Figure 2: Diagrammatic representation of Double Chambered Right Ventricle
Figure 2: Diagrammatic representation of Double Chambered Right Ventricle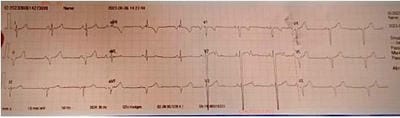 Figure 3: rS complexes from V1- V6, extreme left axis deviation, normal sinus rhythm
Figure 3: rS complexes from V1- V6, extreme left axis deviation, normal sinus rhythm Figure 4: X-ray chest PA. There is cardiomegaly with normal pulmonary blood flow.
Figure 4: X-ray chest PA. There is cardiomegaly with normal pulmonary blood flow. 
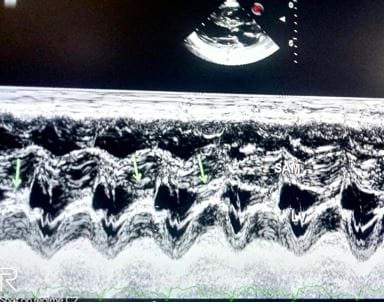 Figure 6: M-mode echocardiogram at the tip of the mitral valve shows that there is systolic anterior motion of mitral leaflets (SAM) towards the ventricular septum causing severe LVOT obstruction.
Figure 6: M-mode echocardiogram at the tip of the mitral valve shows that there is systolic anterior motion of mitral leaflets (SAM) towards the ventricular septum causing severe LVOT obstruction. 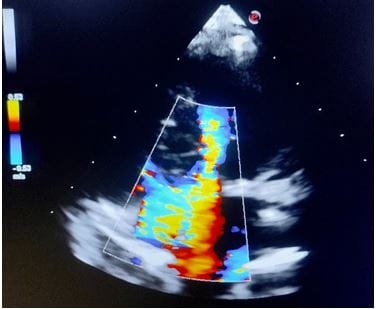 Figure 7: 5 CH View delineates a distinctive mosaic pattern in the LVOT, suggesting severe obstruction across LVOT.
Figure 7: 5 CH View delineates a distinctive mosaic pattern in the LVOT, suggesting severe obstruction across LVOT.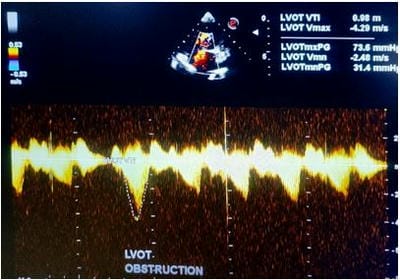 Figure 8: CW Doppler analysis of LVOT shows severe obstruction with a peak/ mean gradient across LVOT being 73.6/ 31.4 mmHg
Figure 8: CW Doppler analysis of LVOT shows severe obstruction with a peak/ mean gradient across LVOT being 73.6/ 31.4 mmHg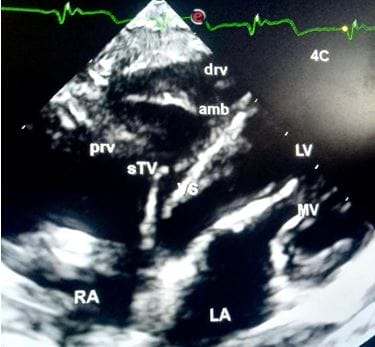 Figure 9. Modified 4 CH View demonstrates the characteristic presence of anomalous muscle bundle (AMB) near the apex of the right ventricle.drv, distal right ventricle, amb, anomalous muscle bundle, prv, proximal right ventricle, sTV, septal leaflet of Tricuspid Valve, VS, ventricular septum, RA, right atrium, LA, left atrium, MV, mitral valve, LV, left ventricle.
Figure 9. Modified 4 CH View demonstrates the characteristic presence of anomalous muscle bundle (AMB) near the apex of the right ventricle.drv, distal right ventricle, amb, anomalous muscle bundle, prv, proximal right ventricle, sTV, septal leaflet of Tricuspid Valve, VS, ventricular septum, RA, right atrium, LA, left atrium, MV, mitral valve, LV, left ventricle. 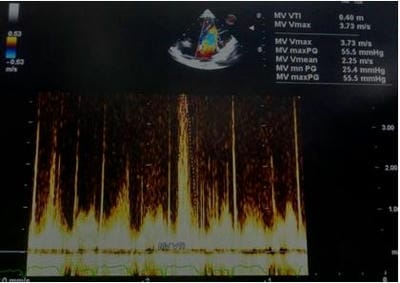 Figure 10: CW Doppler analysis across AMB shows a moderate grade of constriction with a peak/ mean gradient of 55.5/ 25.4 mmHg.
Figure 10: CW Doppler analysis across AMB shows a moderate grade of constriction with a peak/ mean gradient of 55.5/ 25.4 mmHg.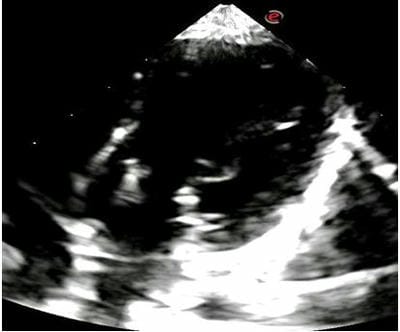 Figure 11: 4 CH View identifies large, thickened and redundant anterior and posterior mitral leaflets at the base of the left ventricular chamber.
Figure 11: 4 CH View identifies large, thickened and redundant anterior and posterior mitral leaflets at the base of the left ventricular chamber. 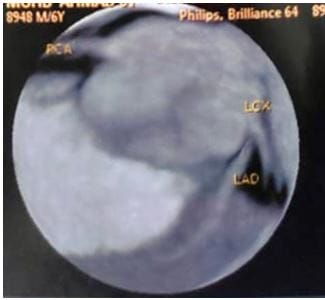 Figure 12: Coronary CT Angiography reveals normal coronary artery origins.
Figure 12: Coronary CT Angiography reveals normal coronary artery origins.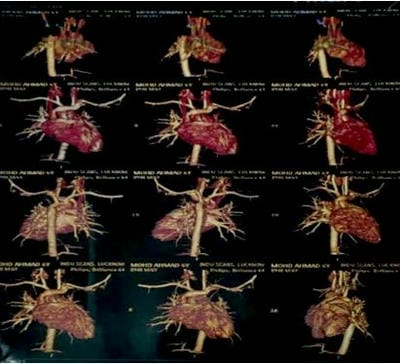 Figure 13: Cardiac CT suggestive of asymmetrical septal hypertrophy with remarkably thickened basal and mid-septum.
Figure 13: Cardiac CT suggestive of asymmetrical septal hypertrophy with remarkably thickened basal and mid-septum.