Association of Plasma Lactate Dehydrogenase concentration with Oxygen Dependence in Newborns with Respiratory Distress
Rahman M.1, Karmaker P.2, Rasel M.3, Tamima Nasrin U.4, Perveen J.5, Afreen S.6, Akhter S.7, Arif Hossain M.8, Abdul Mannan M.9*
DOI: https://doi.org/10.17511/ijpr.2023.i04.01
1 Mahbubur Rahman, Assistant Registrar, Department of Paediatrics, Shaheed M Monsur Ali Medical College & Hospital, Sirajgonj, Bangladesh.
2 Prohlad Karmaker, Assistant Registrar/Assistant Surgeon, Sheikh Sayera Khatun Medical College Hospital, Gopalgonj, Bangladesh.
3 Mohammad Rasel, Assistant Professor, Gonoshasthaya Samaj Vittik Medical College Savar, Savar, Dhaka, Bangladesh.
4 Ummey Tamima Nasrin, Assistant Surgeon, Department of Paediatrics, Upazilla Health Complex, Chandina, Cumilla, Bangladesh.
5 Jahanara Perveen, Consultant, Department of Paediatrics, OSD, DGHS, Dhaka, Bangladesh.
6 Shazia Afreen, Neonatologist, Department of Paediatrics, Kurmitola General Hospital, Dhaka Cantonment, Dhaka, Bangladesh.
7 Shamima Akhter, Medical Officer, Department of Paediatrics, Upazilla Health Complex, Homna, Cumilla, Bangladesh.
8 Md Arif Hossain, Medical Officer, Department of Neonatology, Bangabandhu Sheikh Mujib Medical University (BSMMU), Dhaka, Bangladesh.
9* Md. Abdul Mannan, Professor, Department of Neonatology, Bangabandhu Sheikh Mujib Medical University (BSMMU), Dhaka, Bangladesh.
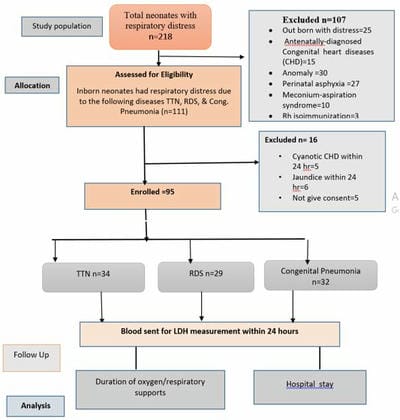
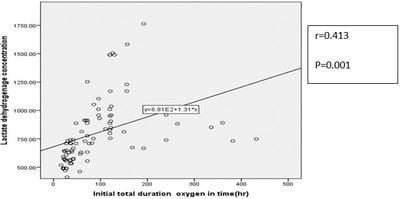
Background: Newborns with respiratory distress may need only supplemental oxygen, whereas those in advanced stages may require other respiratory supports like HHFNC, CPAP, and MV. Methods: This prospective observational study was carried out on 95 neonates, in the Department of Neonatology, BSMMU, Dhaka from July 2021 to June 2022. Enrolled infants were assigned into three groups: RDS group, TTN group, and congenital pneumonia group. LDH collection was done with all aseptic precautions within 24 hours of admission. Different modes of respiratory support were initiated in patients following NICU protocol according to their respiratory severity score. Respiratory supports were titrated according to the infant’s clinical condition, percent saturation of oxygen, and/or arterial blood gas analysis as per NICU protocol. Result: A total of 95 neonates were studied, mean values of LDH among the study groups were 755.64±222.70 u/l, 914.68±304.29 u/l and 742.81±284.70 u/l in TTN, RDS, and congenital pneumonia group respectively. High LDH levels were significantly associated with an increased need for oxygen support in the study group (P=0.04). In subgroup analysis showed high LDH was significantly associated with an increased need for oxygen support in TTN and congenital pneumonia group (P=0.024, P=0.001) respectively. Pearson correlation showed a positive correlation between LDH values and duration of oxygen supports (r=0.413, P=001). In this study, high LDH was also significantly associated with high respiratory support (p=0.001). There was no statistical association found between high LDH and hospital stay (P=0.165). Conclusion: High LDH was associated with the increased need for oxygen and advanced respiratory support among the baby with respiratory distress soon after birth.
Keywords: Plasma Lactate Dehydrogenase, Respiratory Distress, oxygen support
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Professor, Department of Neonatology, Bangabandhu Sheikh Mujib Medical University (BSMMU), Dhaka, , Bangladesh. Email:  |
Mahbubur Rahman, Prohlad Karmaker, Mohammad Rasel, Ummey Tamima Nasrin, Jahanara Perveen, Shazia Afreen, Shamima Akhter, Md Arif Hossain, Md. Abdul Mannan, Association of Plasma Lactate Dehydrogenase concentration with Oxygen Dependence in Newborns with Respiratory Distress. Pediatric Rev Int J Pediatr Res. 2023;10(4):69-77. Available From https://pediatrics.medresearch.in/index.php/ijpr/article/view/754 |
 |
 ©
©