Study of Incidence, Risk Factors and Clinical Profile of Neonatal Hypoglycemia in a Tertiary Care Hospital
Singh P.1*
DOI: https://doi.org/10.17511/ijpr.2023.i04.02
1* Prerana Singh, Senior Resident, Department of Paediatrics, GMC, Mahasamund, Chhattisgarh, India.
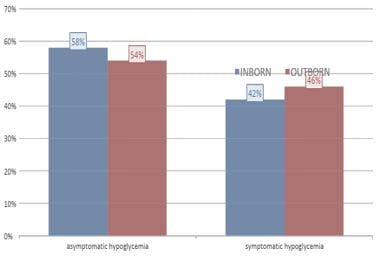
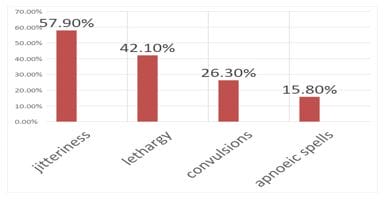
Background: The clinical manifestations of hypoglycemia are non-specific. Studying the incidence, and identifying clinical features and risk factors associated with hypoglycemia, may help in preventing neurological damage. Materials and Methods: This prospective observational study was done over 6 months in GMC Mahasamund. All babies admitted to NICU with whole blood sugar levels <40 mg/dl were subjected to detailed history, thorough clinical examination and observation of signs and symptoms. Results: Neonatal hypoglycemia constituted about 11.7% of the neonates among which 56% were preterm,56% were outborn and 44% were inborn. A greater number of male babies (67%) had hypoglycemia with a male-to-female ratio of 2:1. Asymptomatic hypoglycemia was noticed in 56% and symptomatic in 44%. The major clinical manifestations were jitteriness(57.9%) followed by lethargy(42.1%), convulsions(26.3%) and apnoeic spells(15.8%). We noticed PIH as the most significant maternal risk factor accounting for (37.2%) followed by APH(16.4%). Chronic diabetes mellitus and gestational diabetes were both associated with 4.7% of cases. We found prematurity the most associated neonatal risk factor accounting for 55.8% of cases. Birth asphyxia and IUGR accounted for 21.1% of cases each among inborn babies. Early onset sepsis was found in 41.7% and birth asphyxia in 33.3% among outborn babies. Persistent hypoglycemia was noted in 6.9% of cases. Conclusion: Neonatal hypoglycemia constituted 11.7% of NICU admissions. Proper monitoring of blood glucose levels should be done to plan early treatment and prevent neurological damage.
Keywords: Hypoglycemia, Blood Sugar Levels, Neurological Damage
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Senior Resident, Department of Paediatrics, GMC, Mahasamund, Chhattisgarh, India. Email:  |
Prerana Singh, Study of Incidence, Risk Factors and Clinical Profile of Neonatal Hypoglycemia in a Tertiary Care Hospital. Pediatric Rev Int J Pediatr Res. 2023;10(4):78-85. Available From https://pediatrics.medresearch.in/index.php/ijpr/article/view/756 |
 |
 ©
© 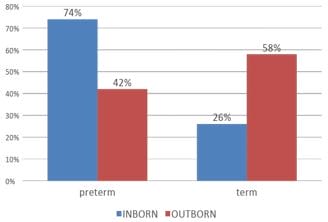
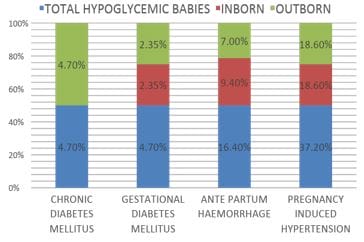
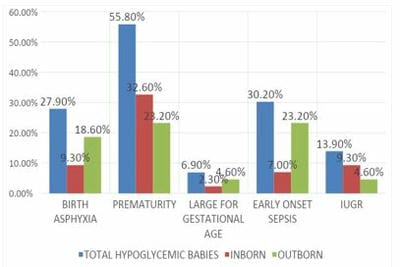 Figure 4: Neonatal risk factors associated with hypoglycemia.
Figure 4: Neonatal risk factors associated with hypoglycemia.