Striking the Right Balance: A Review of Pre-procedural Fasting Protocols and their Impact on Pediatric Patients
Vada S1*, Verma M2, Kumarasamy AP3, Sharma PK4, Kadiyan P5, Anjali A6
https://doi.org/10.17511/ijpr.2024.i03.05
1* Satyam Vada, Msc Nursing, All India Institute of Medical Sciences, Bhopal, Madhya Pradesh, India.
2 Mamta Verma, Associate Professor, Nursing College, All India Institute of Medical Sciences, Bhopal, Madhya Pradesh, India.
3 A P Kumarasamy, Assistant Professor, Nursing College, All India Institute of Medical Sciences, Bhopal, Madhya Pradesh, India.
4 Pramod Kumar Sharma, Head of the Department, Department of Pediatric Surgery, All India Institute of Medical Sciences, Bhopal, Madhya Pradesh, India.
5 Priya Kadiyan, MSc Nursing Student, Department of Nursing, All India Institute of Medical Sciences, Bhopal, Madhya Pradesh, India.
6 Akanksha Anjali, MSc Nursing Student, Department of Nursing, All India Institute of Medical Sciences, Bhopal, Madhya Pradesh, India.
Introduction: Preoperative fasting guidelines have evolved from Sir Joseph Lister's 1883 recommendations to more flexible protocols such as the 1999 American Society of Anaesthesiologists’ 6-4-2 rule and 2022 6-4-1 regimen. Despite these updates, outdated practices still lead to prolonged fasting and related complications.
Aim: This scoping review evaluates current preoperative fasting protocols for Pediatric patients, assesses their impact on outcomes, and identifies areas for improvement to balance aspiration risks with the adverse effects of prolonged fasting.
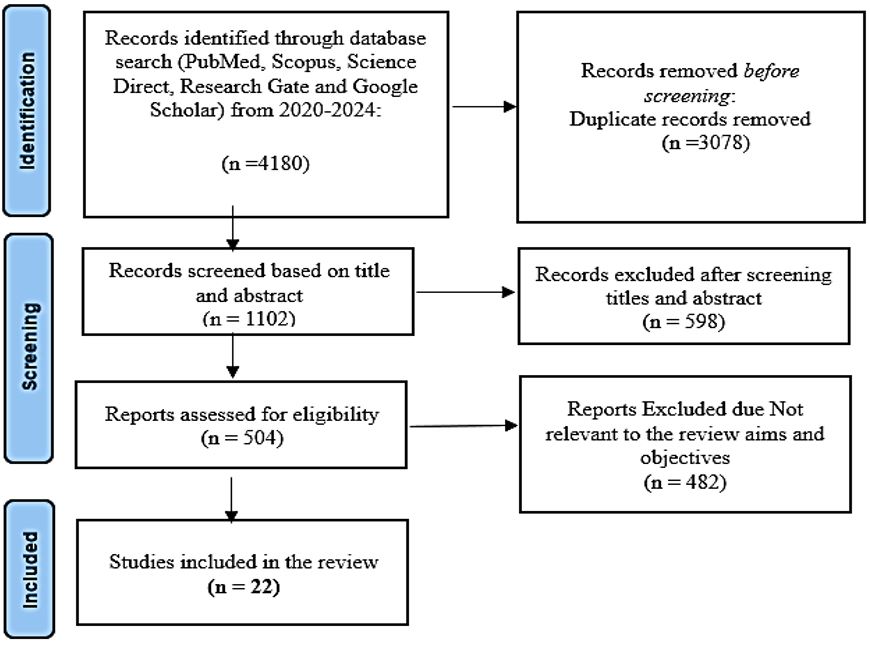
Methodology: An orderly search was conducted across PubMed, Scopus, Science Direct, etc., (up to June 10, 2024) using Boolean operators and keywords like "pre-procedural fasting," "protocols," "children," and "influencing factors" to select relevant studies based on inclusion criteria.
Results: Prolonged fasting, sometimes up to 16 hours, causes discomfort and increases risks of hypotension, nausea, and hypoglycemia. Challenges include outdated practices, unpredictable surgical schedules, and communication gaps, leading to non-compliance and cancellations. Modern guidelines balance benefits and risks by incorporating a better understanding of gastric emptying and child comfort.
Conclusion: Optimizing preoperative fasting for pediatric patients requires flexible protocols, enhanced family education, and improved healthcare team coordination. Continued research and a multidisciplinary approach are essential for refining practices, improving outcomes, and increasing satisfaction.
Keywords: Pre-procedural fasting, fasting protocols, Influencing Factor, Pediatric patients, Perioperative care
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Msc Nursing, , All India Institute of Medical Sciences, Bhopal, Madhya Pradesh, India. Email:  |
Vada S, Verma M, Kumarasamy AP, Sharma PK, Kadiyan P, Anjali A, Striking the Right Balance: A Review of Pre-procedural Fasting Protocols and their Impact on Pediatric Patients. Pediatric Rev Int J Pediatr Res. 2024;11(3):41-48. Available From https://pediatrics.medresearch.in/index.php/ijpr/article/view/772 |
 |
 ©
©