Study of Bone Mineral Density in Transfusion Dependent Thalassemia, its correlation with Biochemical and Hematological parameters: A Cross-Sectional Study
Hegde DG1*, Ghildiyal R2, Sharma S3, Zope S4, Manavi KM5, Ramaswamy M6
DOI:https://doi.org/10.17511/ijpr.2024.i04.01
1* Darshan G Hegde, MD, Department of Pediatrics, Lokmanya Tilak Municipal Medical College and General Hospital, Mumbai, Maharashtra, India.
2 Radha Ghildiyal, MD, Department of Pediatrics, Lokmanya Tilak Municipal Medical College and General Hospital, Mumbai, Maharashtra, India.
3 Sujata Sharma, MD, Department of Pediatrics, Lokmanya Tilak Municipal Medical College and General Hospital, Mumbai, Maharashtra, India.
4 Sadhana Zope, MD, Department of Pediatrics, Lokmanya Tilak Municipal Medical College and General Hospital, Mumbai, Maharashtra, India.
5 Manavi KM, MD, Department of Pediatrics, Lokmanya Tilak Municipal Medical College and General Hospital, Mumbai, Maharashtra, India.
6 Manjunath Ramaswamy, MD, Department of Pediatrics, Lokmanya Tilak Municipal Medical College and General Hospital, Mumbai, Maharashtra, India.
Background: In thalassemic patients, bone disease is an important cause of morbidity. Patients with transfusion-dependent thalassemia (TDT) are susceptible to osteopenia and osteoporosis, the mechanism being multi-factorial. The present study was undertaken to study the prevalence of osteopenia and osteoporosis in TDT patients and describe its correlation with biochemical, hematological profiles.
Method: A total of 84 patients with TDT on regular PRC transfusion and iron chelation therapy aged between 5 and 18 years were enrolled in the study. Bone mineral densities (BMD) were measured by DXA scan (DXA spine/whole body) and categorized into normal, osteopenia and osteoporosis based on the WHO grading system.
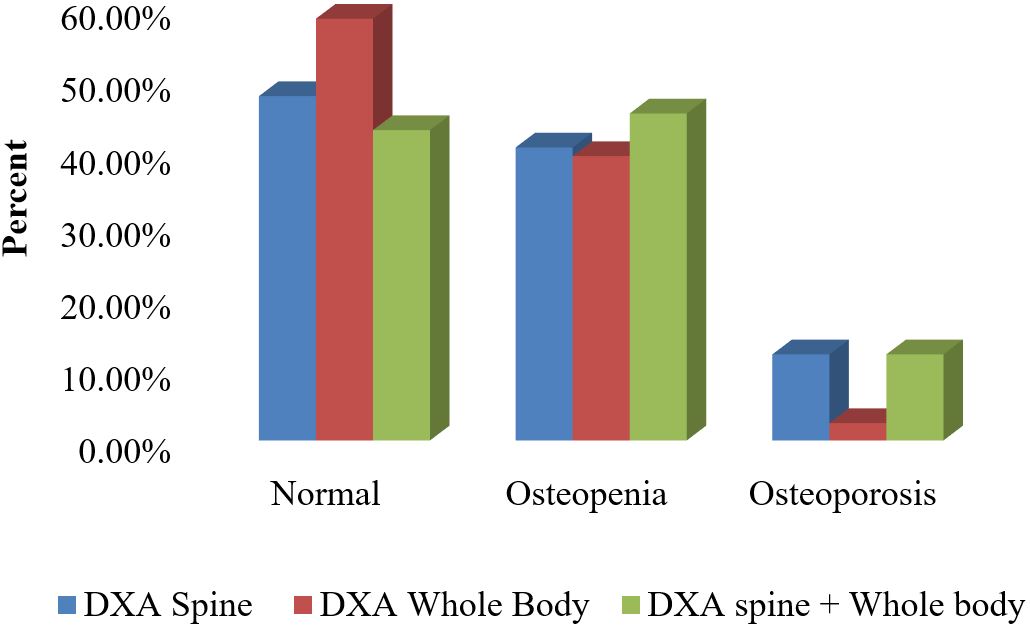
Results: Out of 84 subjects, 57.1% had low BMD with 38(45.2%) having osteopenia and 10(11.9%) of them having osteoporosis. The prevalence of osteoporosis was found to be higher by DXA Spine than by DXA whole body which was found to be statistically significant (P=0.043). A high prevalence of hypoparathyroidism, hypocalcemia, hypovitaminosis D and increased serum phosphorous levels were noted among TDT patients with low BMD. Iron overload in Myocardium by T2*MRI also showed a statistically significant association with low BMD as determined by DXA Spine.
Conclusion: Low bone mass is one of the most prevalent complications among TDT patients. Osteoporosis is a progressive disease with multifactorial etiology. Iron overload status by T2* Cardiac MRI may be used as an early indicator for predicting Osteoporosis along with T-scores from DXA spine for early diagnosis and interventions. Further longitudinal prospective studies are needed to better understand the etiopathogenesis of bone disease in these patients.
Keywords: Transfusion dependant thalassemia, Bone mineral density, Osteoporosis, Osteopenia, DXA scan
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , MD, Department of Pediatrics, Lokmanya Tilak Municipal Medical College and General Hospital, Mumbai, Maharashtra, India. Email:  |
Hegde DG, Ghildiyal R, Sharma S, Zope S, Manavi KM, Ramaswamy M, Study of Bone Mineral Density in Transfusion Dependent Thalassemia, its correlation with Biochemical and Hematological parameters: A Cross-Sectional Study. Pediatric Rev Int J Pediatr Res. 2024;11(4):58-65. Available From https://pediatrics.medresearch.in/index.php/ijpr/article/view/774 |
 |
 ©
©