
Hearing assessment in high-risk neonates by brain stem evoked auditory response (BERA) at a teaching hospital in rural Telangana
Abstract
Introduction: Severe pre-lingual hearing impairment has important consequences for language acquisition, communication, and cognitive, social and emotional development. Indeed evidence is increasing that even moderate hearing loss in very young children can be detrimental. Brainstem evoked response audiometry (BERA), when used and interpreted properly, provide a powerful method of obtaining reliable estimates of auditory sensitivity in infants, young children, and other individuals who cannot or will not provide reliable results on behavioral hearing tests.
Materials & Methods: In this study 110 high risk neonates having one or more risk factors, according to the criteria stated by American Academy of Pediatrics, JCIH 2007 were selected from Newborn unit, of MIMS, Ghanpur. The high risk neonates were subjected to BERA testing in a sound proof room in our study, 30 dB is taken as cutoff for normal auditory threshold.
Results: Mean birth weight of neonates studied was 2.60±0.67 kg. Mean age of neonates at which first BERA done is 19.32±11.3 days. Hyperbilirubinemia requiring Exchange transfusion and TORCH infection were identified as significant risk factors with p-values 0.028 and 0.011 respectively.
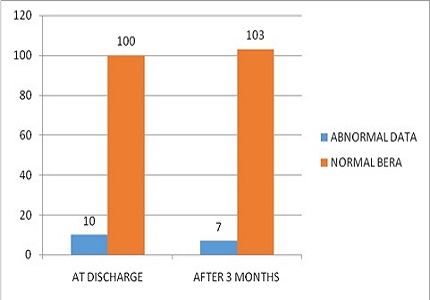
Conclusion: Hearing impairment is common in high risk NICU graduates. Bilateral hearing impairment is more common than unilateral. All high risk infants must be screened for hearing impairment prior to discharge and retesting of infants with abnormal BERA after 3 months and subsequently if necessary. Newborn screening is mandatory to identify hearing loss in the prelinguistic period to reduce the burden of handicap in the community
Downloads
References
2. Taghdiri MM, Eghbalian F, Emami F, Abbasi B, et al. Auditory Evaluation of High Risk Newborns by Automated Auditory Brainstem Response. Iran J Pediatr Dec 2008; 18(4): 330-334. [PubMed]
3. Aiyer RG, Parikh B. Evaluation of auditory brainstem responses for hearing screening of high-risk infants. Indian J Otolaryngol Head Neck Surg. 2009 Mar;61(1):47-53. doi: 10.1007/s12070-009-0034-4. Epub 2009 Mar 31. [PubMed]
4. Robertson CM, Howarth TM, Bork DL, Dinu IA. Permanent bilateral sensory and neural hearing loss of children after neonatal intensive care because of extreme prematurity: a thirty-year study. Pediatrics. 2009 May;123(5):e797-807. doi: 10.1542/peds.2008-2531. [PubMed]
5. Erenberg A, Lemons J, Sia C, Trunkel D, Ziring P. Newborn and infant hearing loss: detection and intervention.American Academy of Pediatrics. Task Force on Newborn and Infant Hearing, 1998- 1999. Pediatrics. 1999 Feb;103(2):527-30. [PubMed]
6. Sukumaran TU. Newborn Hearing Screening Program. Indian Pediatr. 2011 May;48(5):351-3. [PubMed]
7. World Health Organization. WHO: prevention of blindness and deafness.2013. http://www.who.int/pbd/deafnee/hearing_impairment_grades/en/
8. Declau F, Boudewyns A, van den Ende J, Peeters A, Heyning P. Analysis of 170 referred neonates etiologic and audiologic evaluations after universal neonatal hearing screening. Pediatrics. 2008; 121(6):1119-26. [PubMed]
9. Ansari MS. Screening programme for hearing impairment in newborns: A challenge during rehabilitation for all. Asia Pacific disability Rehabilitation Journal. 2004; 15: 83-89.
10. Bilgen H, Akman I, Ozek E, Kulekei S, Ors R, Carman K et al. Auditory brain stem response screening for hearing loss in high risk neonates. Turk J Med Sci. 2000; 30: 479 – 82.
11. Morales SG, Poblano A, Galvan AR, Carrocera LAF. Auditory evoked potentials in children at neonatal risk for hypocusis. Pan Am J Public Health. 1997; 2(4): 232 – 37. [PubMed]
12. Oudesluys-Murphy AM, van Straaten HL, Ens-Dokkum MH, Kauffman-de Boer MA.[Neonatal hearing screening]. Ned Tijdschr Geneeskd. 2000 Mar 25;144(13):594-8. [PubMed]
13. Christine Ohl, Liliane Dornier, Ce´ cile Czajka, Jean-Claude Chobaut, Laurent Tavernier. Newborn hearing screening on infants at risk. International Journal of Pediatric Otorhinolaryngology. 2009;73: 1691–1695 DOI: http://dx.doi.org/10.1016/j.ijporl.2009.08.027. [PubMed]
14. Christiane Meyer , Witte J, Hildmann A, Hennecke KH, Schunck KU, Maul K et al. Neonatal Screening for Hearing Disorders in Infants at Risk: Incidence, Risk Factors, and Follow-up. Pediatrics 1999; 104:900. [PubMed]
15. Zamani A, Daneshjou K, Ameni A, Takand J. Estimating The Incidence Of Neonatal Hearing Loss In High Risk Neonates. Acta Medica Iranica 2004; 42(3):176-180. [PubMed]
16. Gupta AK, Anand NK, Raj H. Evaluation of risk factors for hearing impairment in at risk neonates by brainstem evoked response audiometry (BERA). Indian J Pediatr. 1991 Nov-Dec;58(6):849-55. [PubMed]
17. Bess FH, Humes LE. Structure and function of the auditory system. In Audiology: the fundamentals. 4th ed. Philadelphia: Lippincott Williams and Wilkins; 2009, p.101 – 57.
18. Sawada S, Mori N, Mount RJ, Harrison RV. Differential vulnerability of inner and outer hair cell systems to chronic mild hypoxia and glutamate ototoxicity: insights into the cause of auditory neuropathy. J Otolaryngol. 2001 Apr;30(2):106-14. [PubMed]
19. Vohr BR, Widen JE, Cone-Wesson B, Sininger YS, Gorga MP, Folsom RC, Norton SJ. Identification of neonatal hearing impairment: characteristics of infants in the neonatal intensive care unit and well-baby nursery. Ear Hear. 2000 Oct;21(5):373-82. [PubMed]
20. Agrawal VK, Shukla R, Misra PK, Kapoor RK, Malik GK. Brainstem auditory evoked response in newborns with hyperbilirubinemia. Indian Pediatr. 1998 Jun;35(6):513-8. [PubMed]
21. Sleifer P, da Costa SS, Cóser PL, Goldani MZ, Dornelles C, Weiss K. Auditory brainstem response in premature and full-term children. Int J Pediatr Otorhinolaryngol. 2007 Sep;71(9):1449-56. Epub 2007 Jul 13. [PubMed]
22. Guilhoto LM, Quintal VS, da Costa MT. Brainstem auditory evoked response in normal term neonates. Arq Neuropsiquiatr. 2003 Dec;61(4):906-8. Epub 2004 Jan 6. [PubMed]
23. Roopakala MS, Dayananda G, Manjula P, Konde AS, Acharya PT, Srinivasa R, Nirmala KS. A comparative study of brainstem auditory evoked potentials in preterm and full-term infants. Indian J Physiol Pharmacol. 2011 Jan-Mar;55(1):44-52. [PubMed]
24. Casali RL, Santos MF. Casali RL1, Santos MF. Braz J Otorhinolaryngol. 2010 Nov-Dec;76(6):729-38. [PubMed]
Copyright (c) 2016 Author (s). Published by Siddharth Health Research and Social Welfare Society

This work is licensed under a Creative Commons Attribution 4.0 International License.

 OAI - Open Archives Initiative
OAI - Open Archives Initiative