
Clinical, laboratory profile & antibiotic use in first time Wheezers in the tertiary care centre in the rural area
Abstract
Background: Acute bronchiolitis is primarily due to acute viral infection. There is need for the clinicians to adopt judicious use of antibiotics with understanding of the aetiopathogenesis clinical course, complications and the outcome. It is possible to use the antimicrobials rationally.
Objective: To evaluate the antibiotic requirement from the data collected from the first time wheezers among the hospitalized patients in the pediatric tertiary care centre cum teaching hospital in the rural area. The data was analyzed to justify the antimicrobial use in clinical practice in children with acute bronchiolitis.
Method: This is retrospective study with cross sectional analysis. Data was collected from the patients admitted during the year 2015 January to December, Admission complaints, positive clinical signs, symptoms, and lab investigations were collected to correlate with antibiotic usage in the patients diagnosed as acute bronchiolitis. New symptoms during treatment, duration of stay and outcome were recorded to compare antibiotic group with non antibiotic group. The data was analyzed and compared with other studies.
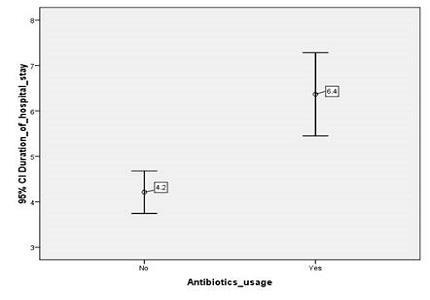
Results: Out of total 70 cases 7 cases were excluded as per exclusion criteria. 63 cases were included in our study. 63 percent of cases are less than 6 months in our study. 71% of cases are males. 47% of cases have received either oral or intravenous antibiotics. The mean duration of stay in antibiotic group is 6.3 days when compared to 4.2 days in non antibiotic group.
Conclusion: with good correlation of clinical and laboratory parameters antibiotic use can be restricted in acute bronchiolitis which is due to acute viral disease.
Downloads
References
2. Putto A, Ruuskanen O, Meurman O. Fever in respiratory virus infections. Am J Dis Child. 1986 Nov;140(11):1159-63. [PubMed]
3. Clinical Signs and Symptoms of Influenza | Health Professionals | Seasonal Influenza (Flu) [Internet]. [cited 2016 Dec 12]. Available from: http://www.cdc.gov/flu/professionals/acip/clinical.htm
4. Vla WVL, Marks MI, Stutman HR. Respiratory syncytial virus puzzle: Clinical features, pathophysiology, treatment, and prevention. J Pediatr. 1992 Oct 1;121(4):503–10.
5. Rambaud-Althaus C, Althaus F, Genton B, D'Acremont V. Clinical features for diagnosis of pneumonia in children younger than 5 years: a systematic review and meta-analysis. Lancet Infect Dis. 2015 Apr;15(4):439-50. doi: 10.1016/S1473-3099(15)70017-4. Epub 2015 Mar 11.
6. Greenes DS, Harper MB. Low risk of bacteremia in febrile children with recognizable viral syndromes. Pediatr Infect Dis J. 1999 Mar;18(3):258-61. [PubMed]
7. Bronchiolitis S on D and M of. Diagnosis and Management of Bronchiolitis. Pediatrics. 2006 Oct 1;118(4):1774–93. [PubMed]
8. Hortal M, Mogdasy C, Russi JC, Deleon C, Suarez A. Microbial agents associated with pneumonia in children from Uruguay. Rev Infect Dis. 1990 Dec;12 Suppl 8:S915-22. [PubMed]
9. Howard WA. Differential Diagnosis of Wheezing in Children. Pediatr Rev. 1980 Feb 1;1(8):239–44.
10. S P, V S, Hk P, J C. Antibiotic prescribing pattern in paediatric in patients with first time wheezing., Antibiotic prescribing pattern in paediatric in patients with first time wheezing. Ital J Pediatr. 2011 Sep 5;37:40. doi: 10.1186/1824-7288-37-40.
11. Liebelt EL, Qi K, Harvey K. Diagnostic Testing for Serious Bacterial Infections in Infants Aged 90 Days or Younger With Bronchiolitis. Arch Pediatr Adolesc Med. 1999 May 1;153(5):525–30.
12. McMillan JA, Tristram DA, Weiner LB, Higgins AP, Sandstrom C, Brandon R. Prediction of the duration of hospitalization in patients with respiratory syncytial virus infection: use of clinical parameters. Pediatrics. 1988 Jan;81(1):22–6. [PubMed]
13. Davies HD, Matlow A, Petric M, Glazier R, Wang EE. Prospective comparative study of viral, bacterial and atypical organisms identified in pneumonia and bronchiolitis in hospitalized Canadian infants. Pediatr Infect Dis J. 1996 Apr;15(4):371–5.
14. Hendaus MA, Alhammadi AH, Khalifa MS, Muneer E, Chandra P. Risk of urinary tract infection in infants and children with acute bronchiolitis. Paediatr Child Health. 2015 Jun-Jul;20(5):e25-9. [PubMed]
15. Kuppermann N, Bank DE, Walton EA, Senac MO, McCaslin I. Risks for Bacteremia and Urinary Tract Infections in Young Febrile Children With Bronchiolitis. Arch Pediatr Adolesc Med. 1997 Dec 1;151(12):1207–14. [PubMed]
16. Andrade MA, Hoberman A, Glustein J, Paradise JL, Wald ER. Acute otitis media in children with bronchiolitis. Pediatrics. 1998 Apr;101(4 Pt 1):617–9. [PubMed]
17. Levine DA, Platt SL, Dayan PS, Macias CG, Zorc JJ, Krief W, et al. Risk of serious bacterial infection in young febrile infants with respiratory syncytial virus infections. Pediatrics. 2004 Jun;113(6):1728–34. [PubMed]
18. Risk of serious bacterial infection in young febrile infants with respiratory syncytial virus infections. [Internet]. [cited 2016 Dec 10]. Available from: http://www.medscape.com/medline/abstract/15173498
19. 611.full.pdf [Internet]. [cited 2016 Dec 13]. Available from: http://thorax.bmj.com/content/61/7/611.full.pdf?61/7/611
20. Friis B, Andersen P, Brenøe E, Hornsleth A, Jensen A, Knudsen FU, et al. Antibiotic treatment of pneumonia and bronchiolitis. A prospective randomised study. Arch Dis Child. 1984 Nov 1;59(11):1038–45.
21. Titus MO, Wright SW. Prevalence of serious bacterial infections in febrile infants with respiratory syncytial virus infection. Pediatrics. 2003 Aug;112(2):282–4.
22. Antonow JA, Hansen K, McKinstry CA, Byington CL. Sepsis evaluations in hospitalized infants with bronchiolitis. Pediatr Infect Dis J. 1998 Mar;17(3):231–6. [PubMed]
23. Bronchiolitis Workup: Approach Considerations, WBC Count and Differential, Sepsis Workup [Internet]. [cited 2016 Dec 12]. Available from: http://emedicine.medscape.com/article/961963-workup#c8
24. Purcell K, Fergie J. Concurrent serious bacterial infections in 912 infants and children hospitalized for treatment of respiratory syncytial virus lower respiratory tract infection. Pediatr Infect Dis J. 2004 Mar;23(3):267–9.
25. Purcell K, Fergie J. Concurrent Serious Bacterial Infections in 2396 Infants and Children Hospitalized With Respiratory Syncytial Virus Lower Respiratory Tract Infections. Arch Pediatr Adolesc Med. 2002 Apr 1;156(4):322–4.
26. Chlamydial Pneumonias: Overview, Pathophysiology, Epidemiology. 2016 Apr 24 [cited 2016 Dec 12]; Available from: http://emedicine.medscape.com/article/297351-overview
27. Indian Pediatrics - Editorial [Internet]. [cited 2016 Dec 13]. Available from: http://www.indianpediatrics.net/apr2003/apr-293-295.htm
Copyright (c) 2016 Author (s). Published by Siddharth Health Research and Social Welfare Society

This work is licensed under a Creative Commons Attribution 4.0 International License.

 OAI - Open Archives Initiative
OAI - Open Archives Initiative