
Congenital adrenal hyperplasia in a male neonate presenting as unresponsive sepsis
Abstract
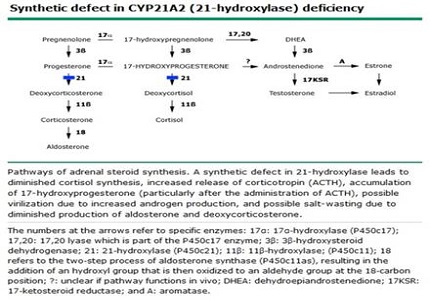
Congenital Adrenal Hyperplasia (CAH) is a disease of Adrenal steroid synthesis. Classic congenital adrenal hyperplasia (CAH) due to 21 hydroxylase deficiency results in one of two clinical syndromes: a salt-losing form or a simple virilizing form. Girls with both forms present with ambiguous genitalia. Newborn males show no overt signs of CAH and so a high index of suspicion is needed to diagnose in them. We report a case of 20 day old male newborn who presented to us in shock which was resistant to routine resuscitative measures. CAH was suspected and was diagnosed based on 17 OH progesterone levels.
Downloads
References
2. Speiser PW, Azziz R, Baskin LS, Ghizzoni L, Hensle TW, Merke DP, Meyer-Bahlburg HF, Miller WL, Montori VM, Oberfield SE, Ritzen M, White PC; Endocrine Society. Congenital adrenal hyperplasia due to steroid 21-hydroxylase deficiency: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2010 Sep;95(9):4133-60. doi: 10.1210/jc.2009-2631.
3. Witchel SF, Nayak S, Suda-Hartman M, Lee PA. Newborn screening for 21-hydroxylase deficiency: results of CYP21 molecular genetic analysis. J Pediatr. 1997 Aug;131(2):328-31. [PubMed]
4. Al-Alwan I, Navarro O, Daneman D, Daneman A. Clinical utility of adrenal ultrasonography in the diagnosis of congenital adrenal hyperplasia. J Pediatr. 1999 Jul;135(1):71-5. [PubMed]
5. Gonzalez RR, Mäentausta O, Solyom J, Vihko R. Direct solid-phase time-resolved fluoroimmunoassay of 17 alpha-hydroxyprogesterone in serum and dried blood spots on filter paper. Clin Chem 1990; 36:1667.
6. Minutti CZ, Lacey JM, Magera MJ, et al. Steroid profiling by tandem mass spectrometry improves the positive predictive value of newborn screening for congenital adrenal hyperplasia. J Clin Endocrinol Metab 2004; 89:3687.
7. Nordenström A, Thilén A, Hagenfeldt L, Larsson A, Wedell A. Genotyping is a valuable diagnostic complement to neonatal screening for congenital adrenal hyperplasia due to steroid 21-hydroxylase deficiency. J Clin Endocrinol Metab. 1999 May;84(5):1505-9.
8. Mornet E, Boue J, Raux-Demay M, et al. First trimester prenatal diagnosis of 21-hydroxylase deficiency by linkage analysis to HLA-DNA probes and by 17-hydroxyprogesterone determination. Hum Genet 1986; 73:358.
Copyright (c) 2017 Author (s). Published by Siddharth Health Research and Social Welfare Society

This work is licensed under a Creative Commons Attribution 4.0 International License.

 OAI - Open Archives Initiative
OAI - Open Archives Initiative