
A study of renal functions in asphyxiated term newborns
Abstract
Introduction: Hypoxia and ischemia can cause damage to almost every tissue and organ in the body. Birth asphyxia is the most important cause of renal damage in term infants. This study was performed to evaluate the renal functions and to compare them with various grades of birth asphyxia in term newborns. This was also compared with levels in healthy term newborns.
Methods: The present study was conducted at the Special Care Neonatal Unit of Mahila Chikitsalaya, SMS Medical College, Jaipur. It was a hospital based comparative analysis conducted from October 2015 to September 2016. It included 100 consecutive term neonates who suffered asphyxia at birth as cases and 50 consecutive healthy term newborns as controls.
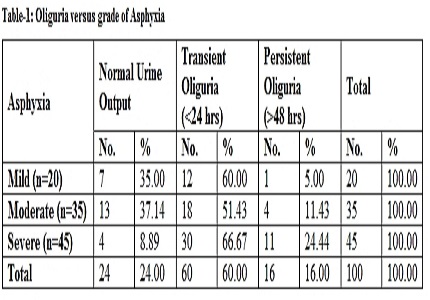
Results: Out of 100 asphyxiated cases, 20% had mild asphyxia (Apgar 6-7), 35% had moderate asphyxia (Apgar 4-5) and 45% had severe asphyxia (Apgar ≤3). Oliguria (Transient and Persistent) was more commonly seen in severely asphyxiated babies as compared to mild asphyxia (p=0.014) and moderate asphyxia (p=0.006). Blood urea and serum creatinine levels on Day 2 and Day 3 of life were significantly raised in severely asphyxiated babies as compared to mildly asphyxiated newborn. The serum electrolytes showed no significant difference among the three categories of asphyxia.
Conclusion: Early estimation of blood urea, serum creatinine and monitoring of urine output should be done in all asphyxiated newborns so that the renal dysfunction can be detected earlier and appropriate measures can be taken in time to prevent renal damage in such newborns.
Downloads
References
2. Dauber IM, Krauss AN, Symchych PS, Auld PA. Renal failure following perinatal anoxia. J Pediatr. 1976 May;88(5):851-55. [PubMed]
3. Mathur NB, Agarwal HS, Maria A. Acute renal failure in neonatal sepsis. Indian J Pediatr. 2006 Jun;73(6):499-02. [PubMed]
4. Perlman JM, Tack ED, Martin T, Shackelford G, Amon E. Acute systemic organ injury in term infants after asphyxia. Am J Dis Child. 1989 May;143(5):617-20. doi:10.1001/archpedi.1989.02150170119037.
5. Darkan AM, Alexender RT. Acute Kidney Injury post neonatal asphyxia. J Pediatr. 2011;158 (2 Suppl):e29-33. doi: 10.1016/j.jpeds.2010.11.010. [PubMed]
6. Ballard JL, Khoury JC, Wedig KL, Wang L, Eilers-Walsman BL, Lipp R . New Ballard Score, expanded to include extremely premature infants. J Pediatr.1991;119(3):417-23.
7. Friedlich PS, Evans JR, Tulassay T, Seri I. Acute and chronic renal failure. In Taeusch HW, Ballard RA, Gleason CA. Avery’s diseases of the newborn. 8th ed. Philadelphia: Elsevier Saunders; 2005. P. 1298-305.
8. Gupta BD, Sharma P, Bagla J, Parakh M, Soni JP. Renal failure in asphyxiated neonates. Indian Pediatr. 2005 Sep;42(9):928-34.
9. Martin-Ancel A, Garcia Alix A, Cabanas F, Burgueros M, Quero J. Multiple organ involvement in prenatal asphyxia. J Pediatr. 1995;127(5):786-93. [PubMed]
10. Olavarría F, Krause S, Barranco L, Herrmann F, Paez V, Mezzano S, Leal N, López M. Renal function in full-term newborns following neonatal asphyxia. A prospective study. Clin Pediatr (Phila). 1987 Jul;26(7):334-38. [PubMed]
11. Ellis M, Manandhar N, Manandhar DS, Del Costello AM. An Apgar score of three or less at one minute is not diagnostic of birth asphyxia but is a useful screening test for neonatal encephalopathy. Indian Pediatr 1998;35(5): 415-21.
12. De Souza SW, Richards B. Neurological sequelae in newborn babies after perinatal asphyxia. Arch Dis Child. 1978 Jul;53(7):564-69. [PubMed]
13. Sarnat HB, Sarnat MS. Neonatal encephalopathy following fetal distress: A clinical and EEG study. Arch Neurol. 1976;33(10): 696-05. [PubMed]
14. Chandra S, Ramji S, Thirupuram S. Perinatal asphyxia: multivariate analysis of risk factors in hospital births. Indian Pediatr. 1997 Mar;34(3):206-12.
15. Daga SR, Fernandes CJ, Soares M, Raote GK, Rao A. Clinical profile of severe birth asphyxia. Indian Pediatr. 1991;28(5): 485-88.
16. Girish Gopal. Acute kidney injury in perinatal asphyxia. Indian J Pharma Biol res. 2014; 2(2): 60-65.
17. Mortazav F, Sakha SH, Nejati N. Acute kidney Failure in Neonatal period. Iranian Journal of Kidney Disease. 2009;3(3):136-40. [PubMed]
18. Low JA, Panagiotopoulos C, Derrick EJ. Newborn complications after intrapartum asphyxia with metabolic acidosis in the term fetus. Am J Obstet Gynecol. 1994 Apr;170(4):1081-87.
Copyright (c) 2017 Author (s). Published by Siddharth Health Research and Social Welfare Society

This work is licensed under a Creative Commons Attribution 4.0 International License.

 OAI - Open Archives Initiative
OAI - Open Archives Initiative