
Prevalence of hypoxemia & its determinates in children with Acute Lower Respiratory infection
Abstract
Introduction: Acute lower respiratory tract infections (LRTIs), most commonly pneumonia, are one of the major reasons for which children are brought to the hospitals. Effective reduction of mortality due to pneumonia is possible if children suffering from pneumonia are treated appropriately and promptly. Hypoxemia is the most serious manifestation and strong risk factor for mortality among children with acute lower respiratory tract infections. Early detection and treatment of hypoxemia is important in the management of these children. So in our study, we tried to determine prevalence of hypoxemia in children with acute respiratory tract infections.
Methods: It was a prospective cross sectional study on 150 children aged 2 months- 60 months with acute respiratory symptoms (<14 days). The children who fulfilled the inclusion criteria were evaluated and examined thoroughly and their data was recorded in a pretested proforma. Statistical analysis was done with IBM SPSS 18.
Results: Present study revealed prevalence of hypoxemia to be 35.3% with no significant correlation of age.
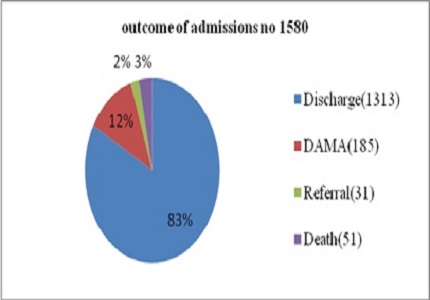
Conclusion: Hypoxemia is present in almost one third of <5 children admitted with acute LRTIs and it is significantly associated with immediate outcome. Therefore sufficient measures should be employed to detect and manage hypoxemia.
Downloads
References
2. Bryce J, Boschi-Pinto C, Shibuya K, Black RE; WHO Child Health Epidemiology Reference Group. WHO estimates of the causes of death in children.Lancet. 2005 Mar 26-Apr 1;365(9465):1147-52.
3. Margolis PA, Ferkol TW, Marsocci S, Super DM, Keyes LL, McNutt R, Harrell FE Jr. Accuracy of the clinical examination in detecting hypoxemia in infants with respiratory illness. J Pediatr. 1994 Apr;124(4):552-60.
4. WHO (199),Health situation in the South-East Asia & Region 1994-1997, Regional office for SEAR, New Delhi.http://www.searo.who.int/entity/health_situation_trends/documents/health_situation_sear_1994-1997.pdf
5. Govt. Of India(2011).Annual report to the people on health. Ministry of Health & Family Welfare, New Delhi.http://mohfw.nic.in/WriteReadData/l892s/6960144509Annual%20Report%20to%20the%20People%20on%20Health.pdf
6. Duke T, Blaschke AJ, Sialis S, Bonkowsky JL. Hypoxaemia in acute respiratory and non-respiratory illnesses in neonates and children in a developing country.Arch Dis Child. 2002 Feb;86(2):108-12.
7. Duke T, Mgone J, Frank D. Hypoxaemia in children with severe pneumonia in Papua New Guinea. Int J Tuberc Lung Dis. 2001 Jun;5(6):511-9.
8. Pocket book of hospital care for children: guidelines for the management of common illnesses with limited resources. 1.Pediatrics 2.Child care 3.Hospitals 4.Child, Hospitalized 5.Developing countries 6.Practice guidelines 7.Manuals I.World Health Organization. ISBN 92 4 154670 0 (NLM classification: WS 29)
9. Leon C, Ricardo A, Stephen M, Mary Fran H. Pediatric Advanced Life Support American Heart Association.Pg no-17.ISBN 13978-1-61669-354-1
10. F-MNCI Facility based integrated management of neonatal and childhood illness. Pg no 111-113.
11. Park K. Parkʾs Textbook of Preventive and Social medicine Bhanot,21st Edition Pg 156.
12. IMNCI- Integrated management of neonatal and childhood illness by WHO and Ministry of Health & Family welfare,Government of India.
13. Lozano JM, Duque OR, Buitrago T, Behaine S. Pulse oximetry reference values at high altitude. Arch Dis Child. 1992 Mar;67(3):299-301.
14. Mwaniki MK, Nokes DJ, Ignas J, Munywoki P, Ngama M, Newton CR, Maitland K, Berkley JA. Emergency triage assessment for hypoxaemia in neonates and young children in a Kenyan hospital: an observational study. Bull World Health Organ. 2009 Apr;87(4):263-70.
15. Morrison B. Anoxia in the acute respiratory infections of childhood; its recognition and treatment. Lancet. 1955 Oct 8;269(6893):737-40.
16. Singhi S, Deep A, Kaur H. Prevalence & predictors of hypoxemia in acute respiratory infections presenting to pediatric emergency department. Indian J Crit Care Med 2003;7:118-123.
17. RakeshLodha, Prateek Singh Bhaduria, AnoopVergheseKuttikat, MadhaviPuranik, Saurabh Gupta, Pandey R M ,Kabra S.K. Can clinical symptoms and signs accurately predict hypoxemia in children with acute lower respiratory tract infections? Indian Pediatrics 2004;41(7):129-135.
18. Made Supartha, PutuSiadiPurniti, RoniNaning , Ida BagusSubanada. Clinical predictors of hypoxemia in 1-5 year old children with pneumonia.PaediatrIndones.2010 ;50:355-60.
Copyright (c) 2015 Author (s). Published by Siddharth Health Research and Social Welfare Society

This work is licensed under a Creative Commons Attribution 4.0 International License.

 OAI - Open Archives Initiative
OAI - Open Archives Initiative