
Study of 99 m-Tc DMSA (Dimercaptosuccinicacid) Scintigraphy in children with urinary tract infection
Abstract
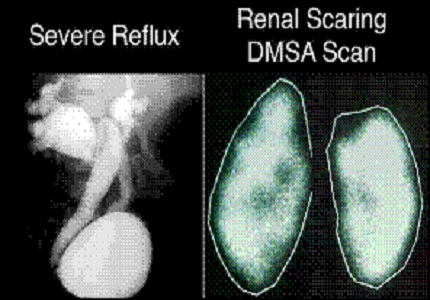
Introduction: DMSA scan is superior to ultrasonography in detecting cortical scars, although the later identifies dilatation of the collecting systems and renal swelling. This study was conducted to know the role of 99m- Tc Dimercaptosuccinic acids (DMSA) scan in children with UTI, its role in the early detection of renal scar.
Materials and Methods: A study was conducted among 125 children at Dr. B.R. Ambedkar Medical College, Bangalore from August 2015- October 2017. The study group included both inpatient and outpatient children with urinary tract infection. The patients with culture positive urinary tract infections during first and recurrent attacks were studied and followed from 3 months to 2 years. On follow- up 99m -Tc DMSA scan was conducted, if needed USG abdomen and MCU scan were conducted.
Results: 44% of the children showed abnormal features both by DMSA scan and USGand 21.6% of the children had normal scan but found to have abnormality in DMSA scan. On follow- up of the children, it was noticed that in 56% of the DMSA scan was normal, in 6% of children who initially had renal scar, on follow up did not have renal scar. 24% of the children persisted to have renal scar on follow up and 12% who initially had normal DMSA scan, on follow up had scar. In that 12 children with renal scar, all the children had VUR grade 4-5.
Conclusion: 99m-Tc DMSA scintigraphy is the gold standard for early identification and evaluation of acute renal inflammation and subsequent renal scarring. This study recommends both renal ultrasound scanning and 99m-Tc DMSA scintigraphy to be routinely performed in infants and children with a first febrile UTI because ultrasonography alone as low sensitivity for the detection of renal cortical abnormalities.
Downloads
References
2. Ross JH, Kay R. Paediatric urinary tract infection andreflux. Am Fam Physician. 1999; 59:1472. [PubMed]
3. Yap Hui Kim. Disorders of the kidney and urinarytract. In: Stanfield P, Brueton M, Waterson T (eds). Disease of children in the subtropics and Tropics.London: Edward Arnold. 1994: 186.
4. Bensman A, Dunand O, Ulinski T. Urinary Tract Infections. In: Ellis D. Avner, William E. Harmon, Patrick Niaudet and NorishigeYosikawa (eds). Pediatric nephrology, 6th edition, Springer Verlag Berlin Heidelberg. 2009;P: 1299-1310.
5. Skoog SJ, Peter CA, Arant BS Jr, Coop HL, Elders JS, Hudson RG et al.Pediatricvesico-ureteral refluxGuidelinePannel Summary Report: Clinical practice guidelines for screening siblings of children withvesico-ureteral reflux neonates/children with prenatal hydronephrosis. J Urol 2010; 184(3):1145- 55.
6. Ransley PG. Vesicoureteric reflux: continuing surgical dilemma. Urology 1978; 12(3):246-55.
7. Dick PT, Feldman W. Routine diagnostic imaging for childhood urinary tract infections: a systematic overview. J Pediatr 1996; 128 (1): 15-22.
8. Aran BS Jr. medical management of mild and moderate vesico-ureteral reflux: follow up studies of infants and young children. A preliminary report of the Southwest Pediatric Nephrology Study Group. J Urol 1992; 48(5): 1683-87.
9. Ozen HA, Whitaker RH. Does the severity of presentation in children with vesico ureteric reflux relate to the severity of the disease or the need for operation? Br J Urol1987;6092): 110-12. [PubMed]
10. Piepsz A. Five year study of medical or surgical treatment in children with vesico ureteral reflux dimercaptosuccinicacid findings. International Reflux Study Group in Europe. Eur J Pediatr 1998;57(9): 753-758.
11. Rosenberg HK, Ilaslan H, Finkelstin MH. Work up of urinary tract infection in infants and children. Ultrasound Q 2001;17(2): 87-102. [PubMed]
12. MacKenzie JR. A review in renal scarring in children. Nucl Med Commun 1996;17(3): 176-190.
13. Jakobsson B, Berg U, Svensson L. Renal scarring after acute pyelonephritis. Archives of Disease in Childhood 1994 :70:111-115. [PubMed]
14. Hellström A, Hanson E, Hansson S, et al. Association between urinary symptoms at 7 years old and previous urinary tract infection. Archives of Disease in Childhood 1991; 66:232-234.
15. Bhagga A, Babu K, Kanitkar M, Srivastava RN.Consensus Statement on management of UTI. Indian Pediatr2001 ; 38:1106-1115. [PubMed]
16. Manish D. Sinha , Paul Gibson.Accuracy of ultrasonic detection of renal scarring in different centres using DMSA as the gold standard Nephrology Dialysis Transplantation ( 2007) 22 : 2213–2216.
17. Nammalwar BR1, Vijayakumar M, Sankar J, Ramnath B , Prahlad N :Evaluation of the use of DMSA in culture positive UTI and culture negative acute pyelonephritis.Indian Pediatr. 2005 Jul;42(7):691-6.
18. Fong KW , Wong SN . Sypmtomatic UTI in children: Experience in a regional Hospital in Hong Kong. HK J Paediatr2004 ; 9 : 30-36.
19. Hewitt IK, Pennesi M, Morello W, Ronfani L, Montini G : Antibiotic Prophylaxis for Urinary Tract Infection-Related Renal Scarring: A Systematic Review.Pediatrics. 2017 May;139(5). pii: e20163145. doi: 10.1542/peds.2016-3145. Epub 2017 Apr 6. [PubMed]
20. Howard RG, Roebuck DJ, Yeung PA, Chan KW, Metreweli C.Vesicoureteric reflux and renal scarring in Chinese children. Br J Radiol. 2001 Apr;74(880):331-4.
21. Benador D, Benador N, Slosman D, Mermillod B, Girardin E: Are younger children at highest risk of renal sequelae after pyelonephritis? Lancet 349: 17–19, 1997.
22. Miguel Zerati Filho; Adriano A. Calado; Ubirajara Barroso Jr; Joao L. Amaro. Spontaneous resolution rates of vesicoureteral reflux in Brazilian children: a 30-year experience. Int. braz j urol. vol.33 no.2 Rio de Janeiro Mar./Apr. 2007.
23. C onway PH, Cnaan A, Zaoutis T, Henry BV, Grundmeier RW, Keren R : Recurrent urinary tract infections in children: risk factors and association with prophylactic antimicrobials.JAMA. 2007 Jul 11;298(2):179-86.
24. Garin EH, Olavarria F, Garcia Nieto V, Valenciano B, Campos A, Young L : Clinical significance of primary vesicoureteral reflux and urinary antibiotic prophylaxis after acute pyelonephritis: a multicenter, randomized, controlled study.Pediatrics. 2006 Mar; 117(3):626-32. [PubMed]
Copyright (c) 2018 Author (s). Published by Siddharth Health Research and Social Welfare Society

This work is licensed under a Creative Commons Attribution 4.0 International License.

 OAI - Open Archives Initiative
OAI - Open Archives Initiative