
A study on clinico-laboratory profile of newborns with perinatal asphyxia admitted to tertiary care hospital
Abstract
Introduction: Asphyxia is the single most important cause of still-births accounting for 45.1% of all cases. Although many organ systems can be affected by hypoxia, it is the nervous system that bears the brunt of perinatal asphyxia in the long run. Once the cerebral injury has occurred, the management is mainly supportive. Newer cerebro protective therapies are being tried. The present study aims at correlating the Severity of asphyxia with the severity of HIE and also to assess the perinatal factors, clinico laboratory profile and immediate outcome in asphyxiated newborns.
Materials and methods: It is a prospective, descriptive clinical study done at NICU, ASRAM medical college Eluru.92 newborn babies who fulfilled the selection criteria for perinatal asphyxia during the study period September 2015 to August 2017 formed the study group.The stage of encephalopathy was assessed according to Sarnat and Sarnat Clinical staging system. Perinatal asphyxia was graded as moderate or severe based on pH and/or Apgarscore.Chi square test and Fisher Exact test has been used to find the significant association of HIE staging and outcome and other study characteristics.
Results: Among 92 asphyxiated newborns, Pregnancy was complicated by the presence of PIH in 15 (16.3%), APH in 3 (3.3%), MSAF was present in 51 (55.4%), maternal anemia in 16 (17.4%) and PROM in 9 (9.8%). Labour was complicated by prolonged II stage in 12 (13.0%) of them and cord prolapse was seen in 1 (1.1%).HIE occurred in 59 (64.13%) out of 92 asphyxiated neonates. According to Sarnat and Sarnat clinical HIE staging, 33 (55.93%) newborns had stage I, 18 (30.51%) had stage II and 8 (13.56%) of the newborns had stage III HIE.Renal involvement occurred in 43 (46.7%) of the total asphyxiated neonates and was the most commonly involved system, next toCNS (64.13%).
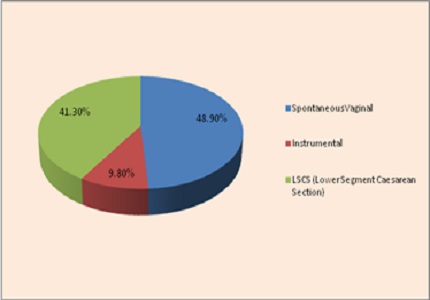
Conclusion: In this study, there is a statistically significant association between severity of perinatal asphyxia and severity of HIE. Apgar score at 1 minute is inversely related to the stages of HIE. Though the neonatal factors like male sex, SGA, LGA and perinatal factors like MSAF, PROM, maternal anemia, LSCS, instrumental delivery and breech presentation are associated with the outcome of HIE (sequelae/death), there is no statistically significant association.
Downloads
References
2. Rajeshwar Reddy A, Praveen Kumar. Follow up of Neonates with Perinatal asphyxia. J Neonatol 2004; 18: 22-27.
3. Vishnu Bhat B, Narayanan P. Birth Asphyxia- Definition and current concepts in management. Indian J PractPediatr 2005; 7: 6-14.
4. Leuthner SR, Das UG. Low Apgar Scores and the definition of birth asphyxia. PediatrClin N Am 2004; 51: 737-745.
5. Cloherty JP, Eichenwald EC, Stark AR. In: Manual of Neonatal care (5thEdn.). Lippincott Williams and Wilkins, Philadelphia. 2004. [PubMed]
6. Martín-Ancel A, García-Alix A, Gayá F, et al. Multiple organ involvement in perinatal asphyxia. J Pediatr. 1995 Nov;127(5):786-93.
7. Chandra S, Ramji S, Thirupuram S. Perinatal asphyxia: multivariate analysis of risk factors in hospital births. Indian Pediatr. 1997 Mar;34(3):206-12. [PubMed]
8. Bernard Rosner (2000), Fundamentals of Biostatistics, 5th Edition, Duxbury.
9. M. Venkataswamy Reddy (2002), Statistics for Mental Health Care Research, NIMHANS publication, INDIA.
10. Gónzalez de Dios J, Moya M. [Perinatal asphyxia, hypoxic-ischemic encephalopathy and neurological sequelae in full-term newborns: an epidemiological study (1)]. Rev Neurol. 1996 Jul;24(131):812-9. [PubMed]
11. Thornberg E, Thiringer K, Odeback A, et al.Birth asphyxia: incidence, clinical course and outcome in a Swedish population. Acta Paediatr. 1995 Aug;84(8):927-32.
12. Robertson C, Finer N. Term infants with hypoxic-ischemic encephalopathy: outcome at 3.5 years. Dev Med Child Neurol 1985; 27: 473-484. [PubMed]
13. Funayama CA, de Moura-Ribeiro MV, Gonçalves AL. [Hypoxic-ischemic encephalopathy in newborn infants. Acute period and outcome]. ArqNeuropsiquiatr. 1997 Dec;55(4):771-9.
14. Peliowski A, Finer NN. Birth Asphyxia in term infant. In: Sinclair JC, Bracken MB (eds). Effective care of the newborn infant. Oxford University Press, Oxford 1992.
15. Portman RJ, Carter BS, Gaylord MS, et al. Predicting neonatal morbidity after perinatal asphyxia: a scoring system. Am J Obstet Gynecol. 1990 Jan;162(1):174-82.
16. Perlman JM, Risser R. Severe fetal acidemia: neonatal neurologic features and short-term outcome. PediatrNeurol 1993; 9: 277-282.
17. Freeman JM, Nelson KB. Intrapartum asphyxia and cerebral palsy. Pediatrics. 1988 Aug;82(2):240-9. [PubMed]
18Murray DM, O'Riordan MN, Horgan R, Boylan G, Higgins JR, Ryan CA.Fetal heart rate patterns in neonatal hypoxic-ischemic encephalopathy: relationship with early cerebral activity and neurodevelopmental outcome.Am J Perinatol. 2009 Sep;26(8):605-12. doi: 10.1055/s-0029-1220774.
19. Perlman JM, Tack ED, Martin T, et al. Acute systemic organ injury in term infants after asphyxia. Am J Dis Child. 1989 May;143(5):617-20.
20. Shah P, Riphagen S, Beyene J, et al. Multiorgan dysfunction in infants with post-asphyxial hypoxic-ischaemic encephalopathy. Arch Dis Child Fetal Neonatal Ed. 2004 Mar;89(2):F152-5. [PubMed]
21. Ramesh S. Pattar, Anil Raj, Bhuvaneshwari Chandrashekhar Yelamali. Incidence of multiorgan dysfunction in perinatal asphyxia. Int J ContempPediatr. 2015 Nov;2(4):428-432. http://dx.doi.org/10.18203/2349-3291.ijcp20150989
22. Malin GL, Morris RK, Khan KS. Strength of association between umbilical cord pH and perinatal and long term outcomes: systematic review and meta-analysis. BMJ. 2010 May 13;340:c1471. doi: 10.1136/bmj.c1471. [PubMed]
23. González de Dios J, Moya M.[Perinatal asphyxia, hypoxic-ischemic encephalopathy and neurological sequelae in full-term newborns. II. Description and interrelation]. Rev Neurol. 1996 Aug;24(132):969-76. [PubMed]
Copyright (c) 2018 Author (s). Published by Siddharth Health Research and Social Welfare Society

This work is licensed under a Creative Commons Attribution 4.0 International License.

 OAI - Open Archives Initiative
OAI - Open Archives Initiative