
A clinical study of pneumonia with special reference to hyponatremia among children aged 1–5 years admitted in teaching hospital
Abstract
Introduction: Pneumonia probably is one of the oldest diseases, as old as antiquity known to human kind and has always remained a subject of challenge to medical science, despite extensive research. Hyponatremia is the most common electrolyte disorder among hospitalized patients and has been associated with increase in mortality.
Objectives: 1) To study clinical profile of pneumonia among children aged 1-5 years. 2) To determine the frequency of hyponatremia in pneumonia.
Methodology: This was a hospital based cross sectional study of pneumonia with special reference to hyponatremia conducted among children aged 1-5 years who were admitted in pediatric wards of Assam Medical College Dibrugarh, Assam, during the period April 2012 to March 2013.
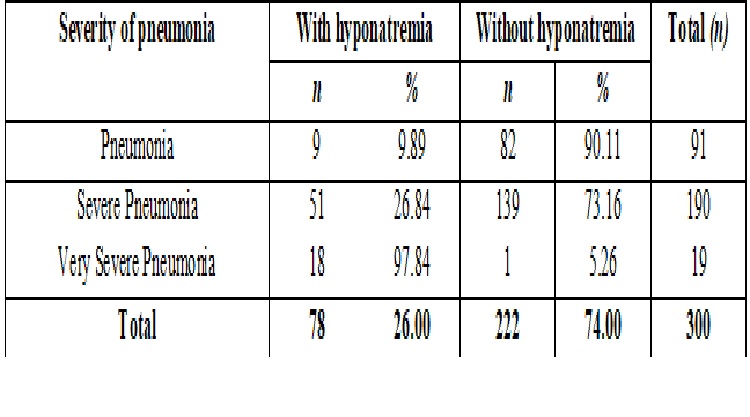
Results: In the present study, outof 300 cases of pneumonia, 78 (26%) cases were hyponatremic. Among them 9 (11.5%) cases were pneumonia, 51 (65.4%) cases were severe pneumonia and 18 (23.1%) cases were very severe pneumonia. Mean duration of hospital stay of patient with hyponatremia with pneumonia was 9.54 ± 2.63 and those with normonatremia with pneumonia were 6.43 ± 1.16.
Conclusion: Incidence of hyponatremia in pneumonia is common and its incidence is more common in cases of very severe pneumonia. Mean duration of hospital stay of patient with hyponatremia with pneumonia is more compared to those with normonatremia with pneumonia.
Downloads
References
2. World Health Organization programme for the control of acute respiratory infections. Acute Respiratory Infections in children: Case Management in small hospitals in developing countries. A manual for doctors and other senior health workers, Geneva: WHO; 2004.
3. Yeates KE, Singer M, Morton AR. Salt and water: a simple approach to hyponatremia. CMAJ. 2004 Feb 3;170(3):365-9.[pubmed]
4. Coenraad MJ, Meinders AE, Vandenbroucke JP, et al. Causes of hyponatremia in the Departments of Internal Medicine and Neurosurgery. Eur J Intern Med. 2003 Aug;14(5):302-309.[pubmed]
5. Nair V, Niederman MS, Masani N, Fishbane S. Hyponatremia in community-acquired pneumonia. Am J Nephrol. 2007;27(2):184-90. Epub 2007 Mar 13.[pubmed]
6. Ellison DH, Berl T. Clinical practice. The syndrome of inappropriate antidiuresis. N Engl J Med. 2007 May 17;356(20):2064-72. doi:10.1056/NEJMcp066837[pubmed]
7. Asadollahi K, Beeching N, Gill G. Hyponatraemia as a risk factor for hospital mortality. QJM. 2006 Dec;99(12):877-80. doi:10.1093/qjmed/hcl120[pubmed]
8. Lussky HO, Friedstein H. Water retension in pneumonia. Amj dis child 1920; 19; 337-43
9. Scott MG, LeGrys VA, Klutts JS. Electrolytes and blood gases.Tietz textbook of clinical chemistry and molecular diagnostics 2006. Saunders WB. Philadelphia. 3rd ed: 983-1018.
10. Reddaiah VP, Kapoor SK. Acute respiratory infections in under five: Experience at comprehensive rural health services project hospital Ballabgarh. Indian J Community Med 1995; 20: 1-4.
11. Sehgal V, Sethi GR, Sachdev HP, Satyanarayana L. Predictors of mortality in subjects hospitalized with acute lower respiratory tract infections. Indian Pediatr. 1997 Mar;34(3):213-9.[pubmed]
12. Drummond P, Clark J, Wheeler J, et al. Community acquired pneumonia--a prospective UK study. Arch Dis Child. 2000 Nov;83(5):408-12.[pubmed]
13. Broor S, Pandey RM, Ghosh M, et al. Risk factors for severe acute lower respiratory tract infection in under-five children. Indian Pediatr. 2001 Dec;38(12):1361-9.[pubmed]
14. Kumar N, Singh N, Locham KK, et al. Clinical evaluation of acute respiratory distress and chest wheezing in infants. Indian Pediatr. 2002 May;39(5):478-83.[pubmed]
15. Gupta D , Mishra S, Chaturvedi P. Fast breathing in the diagnosis of pneumonia--a reassessment. J Trop Pediatr. 1996 Aug;42(4):196-9. doi: 10.1093/tropej/42.4.196.[pubmed]
16. Margolis P, Gadomski A. The rational clinical examination. Does this infant have pneumonia? JAMA. 1998 Jan 28;279(4):308-13.[pubmed]
17. Palafox M, Guiscafré H, Reyes H, et al. Diagnostic value of tachypnoea in pneumonia defined radiologically. Arch Dis Child. 2000 Jan;82(1):41-5.[pubmed]
18. Gadomski AM, Aref GH, Hassanien F, el Ghandour S, el-Mougi M, Harrison LH, et al. Caretaker recognition of respiratory signs in children: Correlation with physical examination findings, x-ray diagnosis and pulse oximetry. Int J Epidemiol 1993; 22: 1166-73.
19. Reddaiah VP, Kapoor SK. Acute respiratory infections in under five: Experience at comprehensive rural health services project hospital Ballabgarh. Indian J Community Med 1995; 20: 1-4.
20. Zilberberg et alBMC Pulmonary Medicine 2008, 8: 16 doi: 10.1186/1471-2466-8-16
21. Singhi S, Dhawan A. Frequency and significance of electrolyte abnormalities in pneumonia. Indian Pediatr. 1992 Jun;29(6):735-40.[pubmed]
Copyright (c) 2018 Author (s). Published by Siddharth Health Research and Social Welfare Society

This work is licensed under a Creative Commons Attribution 4.0 International License.

 OAI - Open Archives Initiative
OAI - Open Archives Initiative