
Etiological profile and outcome and hypertransaminemia in children
Abstract
Objectives: To study the causes of elevated transaminases in children and assess their outcome.
Material and Methods: Retrospective study conducted at Kanchi Kamakoti CHILDS trust hospital, Chennai for 6 months. Medical records of 305children with hypertransaminemia were analyzed for identifying etiology, their utility in diagnosis as well as predicting outcome.
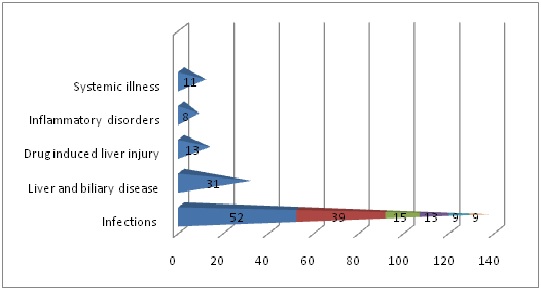
Results: The commonest etiology of elevated transaminases were infections. Highest levels of elevation were recorded in drug induced liver injury and shock. Massive elevation of transaminases along with deranged prothrombin time and albumin was associated with greater mortality and morbidity.
Conclusions: Serum transaminases may be adapted as an improtant investigation, not only to detect liver dysfunction but also to diagnose and prognosticate several disaeses which are non-hepatic in origin.
Downloads
References
2. Thapa BR, Walia A. Liver function tests and their interpretation. Indian J Pediatr. 2007 Jul;74(7):663-71.[pubmed]
3. Ahmar S, Nimain CM. Etiological spectrum of children presenting with raised liver transaminases and their outcome in a tertiary care pediatric facility at Navi Mumbai, India. Clinical Gastroenterology and hepatology. Elsevier Inc. 2015.
4. Davern TJ, Scharschmidt BF. Biochemical liver tests. In: Feidman M, Friedman LS, Sleissenger MH,eds. Sleisenger and Fordtrans Gastrointestinal and liver disease: pathophysiology, diagnosis, management.7th ed. Philadelphia: Saunders; 2002:1227-38.
5. Sorbi D, Boynton J, Lindor KD. The ratio of aspartate aminotransferase to alanine aminotransferase: potential value in differentiating nonalcoholic steatohepatitis from alcoholic liver disease. Am J Gastroenterol. 1999 Apr;94(4):1018-22.doi:10.1111/j.1572-0241.1999.01006.x
6. Iorio R, Sepe A, Giannattasio A, et al. Hypertransaminasemia in childhood as a marker of genetic liver disorders. J Gastroenterol. 2005 Aug;40(8):820-6. DOI:10.1007/s00535-005-1635-7.[pubmed]
7. Wright MA, Yang ML, Parsons JA, et al. Consider muscle disease in children with elevated transaminase. J Am Board Fam Med. 2012 Jul-Aug;25(4):536-40. doi: 10.3122/jabfm.2012.04.110183.[pubmed]
Copyright (c) 2018 Author (s). Published by Siddharth Health Research and Social Welfare Society

This work is licensed under a Creative Commons Attribution 4.0 International License.

 OAI - Open Archives Initiative
OAI - Open Archives Initiative