
Clinical, Bacteriological and Radiological study of severe pneumonia in age group of 2 months to 5 years
Abstract
Background: Acute respiratory infections (ARI) are one of the commonest causes of death in children in developing countries. The future health of children depends on preventing, diagnosing, treating and limiting Acute Lower Respiratory Tract Infection. The use of these clinical signs in the early detection and treatment of children with pneumonia by primary health care workers forms the basis for the case management strategy formulated by the World Health Organization (WHO) to control mortality and morbidity.
Objectives: to study clinical, bacteriological and radiological features of severe pneumonia and to correlate clinical findings with radiological and bacteriological findings.
Materials and Method: A prospective observational study among children between 2 months to 5 years of age. A detailed analysis of symptoms and signs such as fever, cough, rapid breathing, refusal of feeds, wheezing, respiratory rate, presence of fever and other signs of cyanosis, etc were noted. Investigations like Hemoglobin, Total WBC count, Differential WBC count, ESR, blood culture Chest X-ray and if require CT scan were done in all patients. Significance for the statistical tests was predetermined at a probability value of 0.05 or less. (p<0.05)
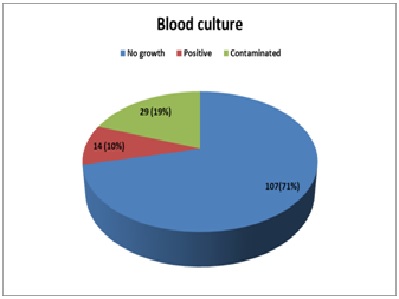
Results: over a period of one and half year total 150 cases were included in the study, nearly all patients were presented with cough, tachypnea, fever, chest retractions and other signs. Positive radiological finding were seen in 80.66% of cases.Among bacterial pneumonia, defined radiologicaly; 63.15% had elevated WBC counts; 88.42% had neutrophilia, 67.27% had elevated ESR. Case fatality rate was 6.3% (9 cases).
Conclusion: clinical diagnosis by WHO ARI criteria are very sensitive and still can be applied to hospitalized children. Chest X-ray is valuable aid in the diagnosis of pneumonia in children
Downloads
References
2. World Health Organization programme for the control of acute respiratory infections. Acute Respiratory Infections in children: Case Management in small hospital in developing countries. A manual for doctors and other senior health workers, Geneva: WHO;2004.
3. World Health Organization programme for the control of acute respiratory infections. Technical bases for the WHO recommendations on management of pneumonia in children at first level health facilities Geneva: WHO;1995.
4. Jadavji T, Law B, Lebel MH, et al. A practical guide for the diagnosis and treatment of pediatric pneumonia. CMAJ. 1997 Mar 1;156(5):S703-11.[pubmed]
5. Revised WHO classification and treatment of childhood pneumonia at health facility: EVIDENCE SUMMARIES. World Health Organization. 2014. from: http://apps.who.int/iris/bitstream/ handle/10665/ 137319/9789241507813_eng.pdf?sequence=1
6. Reddaiah VP, Kapoor SK. Acute respiratory infections in under five: Experience at comprehensive rural health services project hospital Ballabgarh. Indian J Community Med 1995;20:1-4.
7. Sehgal V, Sethi GR, Sachdev HP, Satyanarayana L. Predictors of mortality in subjects hospitalized with acute lower respiratory tract infections. Indian Pediatr. 1997 Mar;34(3):213-9.[pubmed]
8. Drummond P, Clark J, Wheeler J, et al. Community acquired pneumonia--a prospective UK study. Arch Dis Child. 2000 Nov;83(5):408-12.[pubmed]
9. Kumar N, Singh N, Locham KK, Garg R, Sarwal D. Clinical Evaluation of acute respiratory distress and chest wheezing in infants. Indian Pediatrics 2002;39:478-83.
10. Broor S, Pandey RM, Ghosh M, et al. Risk factors for severe acute lower respiratory tract infection in under-five children.Indian Pediatr. 2001 Dec;38(12):1361-9.[pubmed]
11. Gupta D, Mishra S, Chaturvedi P. Fast breathing in the diagnosis of pneumonia--a reassessment. J Trop Pediatr. 1996 Aug;42(4):196-9. doi: 10.1093/tropej/42.4.196.[pubmed]
12. Virkki R, Juven T, Rikalainen H, et al. Differentiation of bacterial and viral pneumonia in children. Thorax. 2002 May;57(5):438-41.[pubmed]
13. Heaton P, Arthur K. The utility of chest radiography in the follow-up of pneumonia. N Z Med J. 1998 Aug 28;111(1072):315-7.[pubmed]
14. Zukin DD, Hoffman JR, Cleveland RH, et al. Correlation of pulmonary signs and symptoms with chest radiographs in the pediatric age group. Ann Emerg Med. 1986 Jul;15(7):792-6.[pubmed]
Copyright (c) 2018 Author (s). Published by Siddharth Health Research and Social Welfare Society

This work is licensed under a Creative Commons Attribution 4.0 International License.

 OAI - Open Archives Initiative
OAI - Open Archives Initiative