
A comparative study of lipid profile in first attack versus relapse cases of idiopathic nephrotic syndrome in children
Abstract
Objectives: Nephrotic dyslipoprotenemia usually revert to normal with remission but hyperlipidemia is a well known risk factor of atherosclerosis and glomerular injury in children. There are few studies comparing the spectrum of dyslipidemia in initial attack and subsequent relapses of nephritic syndrome. The aim of the study was to compare the lipid profile in first attack and relapse cases of Idiopathic Nephrotic Syndrome in children.
Methodology: The prospective study was conducted between May 2015-June 2017 at S.V.P.P.G.I and S.C.B Medical College, Cuttack. Total of 55 cases of Idiopathic Nephrotic Syndrome of aged 1 to 14 years were included in the study. Out of 55 cases 30 cases were in first attack and 25 cases were in the relapses group. The demographic data, lipid profile, magnitude of hyperlipidemia and serum albumin were analyzed in the study.
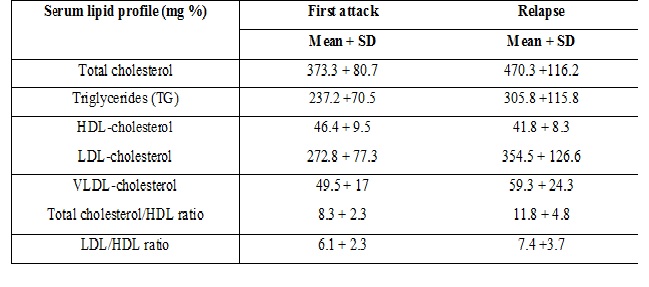
Results: The total serum cholesterol level (470 + 116) mg/dl was higher in relapse cases as compared to first attack group. Similarly serum TG (305+115) mg/dl, LDL (354+126) mg/dl, VLDL (59+24) mg/dl level was higher in relapse cases. However serum HDL (41+8) mg/dl was found to be lower in relapse group as compared to first attack. The serum Albumin level (<2.5gm/dl) was low in all cases but in 12% cases (n=4) of relapse group was very low (<1.0 gm/dl).
Conclusion: This establishes a higher serum cholesterol, TG, LDL, VLDL and marginally lower HDL level in relapse group as compared to first attack which may be explained by lower serum Albumin level causing higher lipid profile. This emphasis the need of close monitoring of lipid profile and in all further episode of relapse group for dietary modification and early intervention.
Downloads
References
2. Marsh JB. Lipoprotein metabolism in the nephrotic syndrome. Front Biosci. 2002 Aug 1;7:e326-38.[pubmed]
3. Appel GB, Blum CB, Chien S, et al. The hyperlipidemia of the nephrotic syndrome. Relation to plasma albumin concentration, oncotic pressure, and viscosity. N Engl J Med. 1985 Jun 13;312(24):1544-8.DOI:10.1056/NEJM198506133122404.
4. Gheradi E, Rota E, Calandra S et al.Relationship among the concentration of serum lipoproteins and changes in their chemical composition in patients with untreated nephrotic syndrome. Eur J Clin Invest, 1997; 7:567-570.
5. Gaston Zilleruelo, Sung L. Hsia, Michael Freundlich,Helen M. Gorman,Jose Strauss. Persistence of serum lipid abnormalities in children with idiopathic nephrotic syndrome, January 1984,volume 104,issue 1, pages 61-64, DOI: https://doi.org/10.1016/S0022-3476(84)80590-9
6. Kamanna VS, Bassa BV, Ganji SH. Low density lipoproteins transactivate EGF receptor: role in mesangial cell proliferation. Life Sci. 2008 Oct 24;83(17-18):595-601. doi: 10.1016/j.lfs.2008.08.010. Epub 2008 Sep 6.[pubmed]
7. Varley H, Gowenlock AH, Bell M. Practical Clinical Biochemistry. Fifth Edition; Jaypee Brothers. India.1991:1:126-8.
8. Searcy RL, Bergquist LM. A new color reaction for the quantitation of serum cholesterol. Clin Chim Acta. 1960 Mar;5:192-9.[pubmed]
9. Fletcher MJ. A colorimetric method for estimating serum triglycerides. Clin Chim Acta. 1968 Nov;22(3):393-7.[pubmed]
10. Stewart JC. Colorimetric determination of phospholipids with ammonium ferrothiocyanate. Anal Biochem. 1980 May 1;104(1):10-4.[pubmed]
11. Consensus Statement on management of steroid sensitive nephritic syndrome. Indian Pediatric Nephrology Group, Indian Academy of Pediatrics. Indian Pediatric 2001; 38:975-986.
12. Walter Heymann, Sudesh P. Makker, The Idiopathic Nephrotic Syndrome of Childhood, A Clinical Re evaluation of 148 Cases Am J Dis Child. 1974;127(6):830-837. doi:10.1001/archpedi.1974.02110250056008
13. Srivastava RN, Bagga A. Nephrotic syndrome in :Pediatric Nephrology.4th edition .2005:161-200
14. Mahmud S, Jahan S, Hossain MM. Hyperlipidemia in childhood idiopathic nephrotic syndrome during initial remission and relapse. Mymensingh Med J. 2011 Jul;20(3):402-6.[pubmed]
15. Arije A, Erasmus RT, Anjorin SA. Plasma lipids and lipoproteins cholesterol distributions in nephrotic syndrome patients during short term steroid treatment. Cent Afr J Med. 1993;39:211-5.
16. Dnyanesh DK, Suma Dnyanesh , Varadaraj Shenoy. A Study of Serum Lipids in Nephrotic Syndrome in Children. IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-ISSN: 2279-0853, p-ISSN: 2279-0861.Volume 13, Issue 3 Ver. I. (Mar. 2014), PP 01-06,
17. Merouani A, Levy E, Mongeau JG, Robitaille P, Lambert M, Delvin EE. Hyperlipidemic profiles during remission in childhood idiopathic nephrotic syndrome. Clinic Biochem. 2003;36:571-4.
18. Moorhead JF, Chan MK, El-Nahas M, et al. Lipid nephrotoxicity in chronic progressive glomerular and tubulo-interstitial disease. Lancet. 1982 Dec 11;2(8311):1309-11.[pubmed]
19. Elzouki AY. Immunological aspect of primary nephrotic syndrome in childhood. Saudi J Kidney Dis and Transplant 1994;5:483-8
20. Meadow SR, Sarsfield JK, Scott DG, et al, Steroid-responsive nephrotic syndrome and allergy: immunological studies. Archives of Disease in Childhood 1981;56:517-524.
21. R.H.RWhite,E.FGlasgow,R.JMills,clinicopathological study of nephrotic syndrome in childhood,The Lancet ,Volume 295, Issue 7661, 27 June 1970, Pages 1353-1359
22. Srivastava RN, Mayekar G, Anand R, et al. Nephrotic syndrome in indian children. Arch Dis Child. 1975 Aug;50(8):626-30.[pubmed]
23. Kaysen GA, Davies RW.Reduction in proteinuria attenuates hyperlipidemia in the nephrotic syndrome. J Am Soc Nephrol.1990;1(suppl 2):S75-79
24. Thomas EM, Rosenblum AH, Lander HB, et al. Relationships between blood lipid and blood protein levels in the nephrotic syndrome. AMA Am J Dis Child. 1951 Feb;81(2):207-14.[pubmed]
25. Krishnaswamy D, Indumati V, Sathishkumar D, Vijay V, Shekanawar M. Serum proteins, initial and follow up lipid profile in children with nephrotic syndrome. Int J Applied Bio Pharma Tech. 2011;2:59-64.
Copyright (c) 2018 Author (s). Published by Siddharth Health Research and Social Welfare Society

This work is licensed under a Creative Commons Attribution 4.0 International License.

 OAI - Open Archives Initiative
OAI - Open Archives Initiative