
Effect of neonatal hyper bilirubinemia on brain stem auditory evoked response
Abstract
Introduction: Neonatal hyperbilirubinemia is a major cause of morbidity in neonates. The long term neurological sequel can be prevented and reversed by timely and aggressive management of hyperbilirubinemia. Brain stem auditory evoked response (BAER) is an assessment tool to help predictimpeding bilirubin neurotoxicity. This study was conducted to evaluate the effect of hyperbilirubinemia on auditory system of newborn and the effect of therapy on BAER.
Materials and Methods: In this case control study, 50 term neonates with hyperbilirubinemia (total serum bilirubin > 15 mg/dl) were included in the study group and 25 normal term neonates were taken as controls. Baseline BAER was recorded in study group before therapy and after therapy. Results were compared with controls and intra group comparison was also done. Continuous data with normal distribution was analysed by student t-test, and categorical data was analysed using chi-square test.
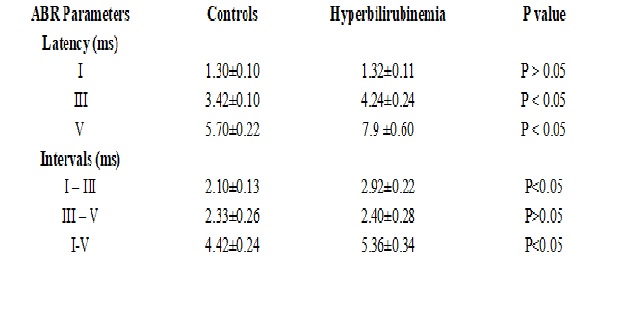
Results: Most common BAER abnormality noted in jaundiced neonates was prolonged latency of wave V (42%) andprolonged inter wave interval I–V (32%). Significant increase in the absolute latencies of waves III and V was noted in hyperbilirubinemic neonates as compared to controls (p<0.05). I-III and I-V inter-peak latencies were also significantly prolonged in neonates with hyper bilirubinemia (p<0.05). There was significant improvement in the latency of wave III and wave V, I – III inter- peak latency and I – V inter-peak latency after treatment (P<0.05).
Conclusion: Results of our study demonstrate the importance of early ABR screening as an efficient tool for monitoring the neonates at risk of bilirubin neurotoxicity. Diagnosing the early changes in ABR caused by hyperbilirubinemia before appearance of clinical abnormality will help prevent bilirubin neurotoxicity.
Downloads
References
2. Connolly AM, Volpe JJ. Clinical features of bilirubin encephalopathy. Clin Perinatol. 1990 Jun;17(2):371-9.[pubmed]
3. Olds C, Oghalai JS. Audiologic impairment associated with bilirubin-induced neurologic damage. SeminFetal Neonatal Med. 2015 Feb;20(1):42-46. doi: 10.1016/j.siny.2014.12.006. Epub 2015 Jan 7.[pubmed]
4. Smith CM, Barnes GP, Jacobson CA, Oelberg DG. Auditory brainstem response detects early bilirubin neurotoxicity at low indirect bilirubin values. J Perinatol. 2004; 24:730–2.[pubmed]
5. Jiang ZD, Zhang L, Wu YY, et al. Brainstem auditory evoked responses from birth to adulthood: development of wave amplitude. Hear Res. 1993 Jun;68(1):35-41.[pubmed]
6. Karmel BZ, Gardner JM, Zappulla RA, Brain-stem auditory evoked responses as indicators of early brain insult. Electroencephalogr Clin Neurophysiol. 1988 Nov-Dec;71(6):429-42.[pubmed]
7. American Academy of Pediatrics Subcommittee on Hyperbilirubinemia. Management of hyperbilirubinemia in the newborn infant 35 or more weeks of gestation. Pediatrics. 2004 Jul;114(1):297-316.[pubmed]
8. Oudesluys-Murphy AM, Harlaar J. Neonatal hearing screening with an automated auditory brainstem response screener in the infant's home. Acta Paediatr. 1997 Jun;86(6):651-5.[pubmed]
9. Watchko JF. Neonatal hyperbilirubinemia--what are the risks? N Engl J Med. 2006 May 4;354(18):1947-9. DOI:10.1056/NEJMe068053.[pubmed]
10. Shapiro SM. Bilirubin toxicity in the developing nervous system. Pediatr Neurol. 2003 Nov;29(5):410-21.[pubmed]
11. Smitherman H, Stark AR, Bhutani VK. Et al. Early recognition of neonatal hyperbilirubinemia and its emergent management. SeminFetal Neonatal Med. 2006 Jun;11(3):214-24. DOI:10.1016/j.siny.2006.02.002.
12. Vohr BR. New approaches to assessing the risks of hyperbilirubinemia. Clin Perinatol. 1990 Jun;17(2):293-306.[pubmed]
13. Vohr BR, Barry L, Rapisardi G, O’Dea C, Brown L, Peucker M et al.Abnormal brain stem function (brain-stem auditory evoked response) correlates with acoustic cry features in term infants with hyperbilirubinemia.The Journal of Paediatr. 1989 Aug; 115(2): 303-8.
14. Palmer C, Smith MB. Assessing the risk of kernicterus using nuclear magnetic resonance. Clin Perinatol. 1990 Jun;17(2):307-29.[pubmed]
15. Hansen TW. Bilirubin brain toxicity. J Perinatol. 2001 Dec;21 Suppl1:S48-51; discussion S59-62. DOI:10.1038/sj.jp.7210634.[pubmed]
16. Sharma R, Grover N, Sankhyan N, Sharma ML. Auditory brainstem responses in neonatal hyperbilirubinemia and effect of therapy. Indian J. Otolaryngol Head Neck Surg. 2006 Oct; 58(4):340-42.
17. Rattay F, Danner SM. Peak I of the human auditory brainstem response results from the somatic regions of type I spiral ganglion cells: evidence from computer modeling. Hear Res. 2014 Sep;315:67-79. doi: 10.1016/j.heares.2014.07.001. Epub 2014 Jul 11.[pubmed]
18. Deorari AK, Singh M, Ahuja GK, et al. One year outcome of babies with severe neonatal hyperbilirubinemia and reversible abnormality in brainstem auditory evoked responses. Indian Pediatr. 1994 Aug;31(8):915-21.[pubmed]
19. Funato M, Teraoka S, Tamai H, et al. Follow-up study of auditory brainstem responses in hyperbilirubinemicnewborns treated with exchange transfusion. Acta PaediatrJpn. 1996 Feb;38(1):17-21.[pubmed]
20. Agrawal VK, Shukla R, Misra PK, et al. Brainstem auditory evoked response in newborns with hyperbilirubinemia. Indian Pediatr. 1998 Jun;35(6):513-8.[pubmed]
21. Perlman M, Fainmesser P, Sohmer H, Tamari H, Wax Y, Pevsmer B. Auditory nerve-brainstem evoked responses in hyperbilirubinemic neonates. Pediatrics. 1983; 72(5):658-64. 37.
22. Shapiro SM. Acute brainstem auditory evoked potential abnormalities in jaundiced Gunn rats given sulphonamide. Pediatr Res. 1988; 23(3):306-10. 38.
23. Shapiro SM. Reversible brainstem auditory evoked potential abnormalities in jaundiced Gunn rats given sulfonamide. Pediatr Res. 1993 Nov;34(5):629-33. DOI:10.1203/00006450-199311000-00014.
24. Gupta AK, Raj H, Anand NK. Auditory brainstem responses (ABR) in neonates with hyperbilirubinemia. Indian J Pediatr. 1990 Sep-Oct;57(5):705-11.[pubmed]
25. Sharma P, Chhangani N, Meena KR, Jora R, Sharma N, Gupta B. Brainstem evoked response audiometry (BAER) in neonates with hyperbilirubinemia. Indian J Pediatr. 2006; 73(5):413-6.

 OAI - Open Archives Initiative
OAI - Open Archives Initiative