
Profile of Ventilator Associated Pneumonia in Children Admitted to Pediatric Intensive Care Unit of a Tertiary Care Center in India
Abstract
Introduction: Limited literature is available on VAP in children, particularly from India.Hence this study aims to determine the incidence, clinical, laboratory, radiological and microbiological profile, risk factors, and outcomes of ventilator-associated pneumonia in pediatric patients.
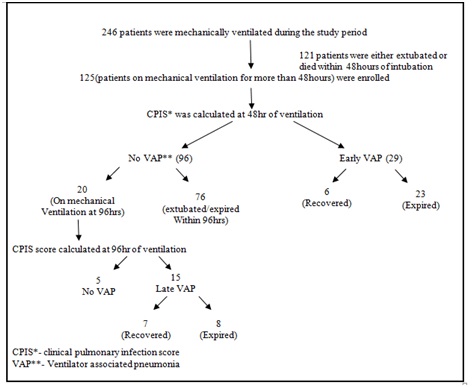
Methods: This is a prospective observational study which enrolled 125 children who were mechanically ventilated in the PICU of a tertiary teaching care hospital over a period of 2 years. Demographic, clinical, radiological and laboratory details were collected and CPIS was used to diagnose VAP. Endo tracheal aspirates were obtained at 48hrs and 96 hrs of initiation of mechanical ventilation and were cultured as per standard guidelines. All the demographic, clinical, radiological and micro biological details were entered in SPSS version 17.0.Standard statistical tests were used to analyze data.
Results: Among the 125 ventilated children, 44 were found to have VAP as per the CPIS showing its incidence of 35.2%. In our study incidence of early VAP is 27.6% while that of late VAP is 75%. The major risk factor for the incidence of VAP in this study was the duration of ventilation. VAP occurred in 75% of patients intubated for more than 5 days. Among 63 children who were reintubated, 34(53.9%) developed VAP while the incidence of VAP was only 16.1% among those who were not reintubated (p value- 0.016). In this study out of the microorganisms isolated in patients with early VAP, 45% were Acinetobacter species, 20% Klebsiella pneumoniae and 10% Pseudomonas aeruginosa. Whereas in late onset VAP, Acinetobacter constituted 60% of all microbes while the rest comprised of Pseudomonas aeruginosa (20%) and Klebsiella pneumonia (6.6%).
Conclusions: Significant risk factors in development of VAP were reintubation and duration of ventilation. The most common VAP pathogen was Acinetobacter species.Tracheostomized children have higher incidence of VAP but have higher recovery rates.
Downloads
References
2. Cooper VB, Haut C. Preventing ventilator-associated pneumonia in children: an evidence-based protocol. Crit Care Nurse. 2013 Jun;33(3):21-9; quiz 30. doi: 10.4037/ ccn 2013204.
3. Hamid MH, Malik MA, Masood J, et al. Ventilator-associated pneumonia in children. J Coll Physicians Surg Pak. 2012 Mar;22(3):155-8. doi: 02.2012/JCPSP. 155158.
4. Sachdev A, Chugh K, Sethi M, et al. Clinical Pulmonary Infection Score to diagnose ventilator-associated pneumonia in children. Indian Pediatr. 2011 Dec;48 (12):949-54. Epub 2011 Mar 15.
5. Venkatachalam V, Hendley JO, Willson DF. The diagnostic dilemma of ventilator-associated pneumonia in critically ill children. PediatrCrit Care Med. 2011 May;12 (3): 286-96. doi:10. 1097/ PCC.0b013e3181fe2ffb.
6. Lodha R, Kabra SK. Diagnosis of Ventilator Associated Pneumonia: Is There a Simple Solution? Indian Pediatrics 2011; 48:939-941
7. Joseph NM, Sistla S, Dutta TK, et al. Ventilator-associated pneumonia in a tertiary care hospital in India: incidence and risk factors. J Infect Dev Ctries. 2009 Dec 15;3(10):771-7.
8. Grasso F, Chidini G, Napolitano L, Calderini E. Ventilator-associated pneumonia in children: evaluation of clinical pulmonary infection score in monitoring the course of illness. Crit Care. 2004;8(Suppl 1):P209. doi: 10.1186/cc2676
9. Gauvin F., Dassa C., Chaïbou M., Proulx F., Farrell C.A., Lacroix J. Ventilator-associated pneumonia in intubated children: Comparison of different diagnostic methods. Pediatr. Crit Care Med. 2003;7:437–443. doi: 10. 1097/01.PCC.0000090290.53959.F4.
10. Raymond J, Aujard Y. Nosocomial infections in pediatric patients: a European, multicenter prospective study. European Study Group. Infect Control Hosp Epidemiol. 2000 Apr; 21 (4):260-3.DOI:10.1086/501755
11. Patra PK, Jayashree M, Singhi S, et al. Nosocomial pneumonia in a pediatric intensive care unit. Indian Pediatr. 2007 Jul;44(7):511-8.
12. Sharma H, Singh D, Pooni P, Mohan U. A study profile of ventilator associated pneumonia in children in Punjab. J Trop Pediatr. 2009;55:393-5.
13. Silva DC, Shibata AR, Farias JA, et al. How is mechanical ventilation employed in a pediatric intensive care unit in Brazil? Clinics (Sao Paulo). 2009; 64 (12): 1161-6. doi: 10.1590/S1807-5932200900 1200005.
14. Shirly GFA, Lakshmi S, Shanthi S, Darlington CD, Vinoth S. Clinical profile of children mechanically ventilated in a paediatric intensive care unit of a limited resource setting. Int J ContempPediatr2016;3:542-5.
15. Awasthi S, Tahazzul M, Ambast A, Govil YC, Jain A. Longer duration of mechanical ventilation was found to be associated with ventilator-associated pneumonia in children aged 1 month to 12 years in India. J Clin Epidemiol. 2013;66:62-6.
16. Bilan N, Habibi, P. Does Re-intubation Increased Risk of Ventilator-Associated Pneumonia (VAP) in Paediatric Intensive Care Unit Patients? Int J Pediatr. 2015; 3:411-5.
17. Galal YS, Youssef MR, Ibrahiem SK. Ventilator-Associated Pneumonia: Incidence, Risk Factors and Outcome in Paediatric Intensive Care Units at Cairo University Hospital. J Clin Diagn Res. 2016 Jun;10 (6): SC06-11. doi: 10.7860/JCDR/2016/ 18570. 7920. Epub 2016 Jun 1.
18. Vincent JL, Marshall JC, Namendys-Silva SA, et al. Assessment of the worldwide burden of critical illness: the intensive care over nations (ICON) audit. Lancet Respir Med. 2014 May;2(5):380-6. doi: 10.1016/S2213-2600(14)70061-X. Epub 2014 Apr 14.
19. Vincent JL, Rello J, Marshall J, et al. International study of the prevalence and outcomes of infection in intensive care units. JAMA. 2009 Dec 2;302(21):2323-9. doi: 10.1001/jama.2009.1754.
20. Bigham MT, Amato R, Bondurrant P, et al. Ventilator-associated pneumonia in the pediatric intensive care unit: characterizing the problem and implementing a sustainable solution. J Pediatr. 2009 Apr;154(4):582-587.e2. doi:10.1016/j.jpeds.2008. 10. 019. Epub 2008 Dec 3.
Copyright (c) 2019 Author (s). Published by Siddharth Health Research and Social Welfare Society

This work is licensed under a Creative Commons Attribution 4.0 International License.

 OAI - Open Archives Initiative
OAI - Open Archives Initiative