
Evaluation of serum LDHlevels in the diagnosis and inmonitoring the response to the treatment in children with megaloblastic anaemia
Abstract
Background: Megaloblastic anaemia is still a common and preventable cause of anaemia in children.Invasive procedure like bone marrow examination and expensive investigation like estimation of serum vitamin B12 and folic acid levels are the definitive diagnostic tools. Their non availability at peripheral centre lead to a great deal of interest in other simple biochemical investigations like estimation of serum LDH levels.
Design/methods: Children aged between 6 months to 14 yrs with clinically suspected megaloblastic anaemia formed the study group. A detailed clinical history and examination was done.All subjects had complete blood counts. Serum LDH levels, serum levels of vitamin B12 and folic acid levels were done. Serial measurements of serum LDH levels were done on day 14 and day 30 of treatment and were correlated with the haemoglobin and MCV levels.
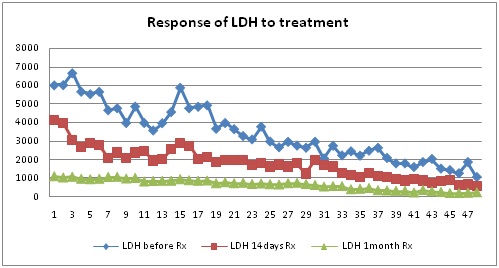
Results:A total of 48 patients formed the study group. All cases were anaemic with mean HB level of 5.25g/dl, mean MCV was 100.15fl. All cases had megaloblastic changes on peripheral smear.42 cases had low vitamin B12 levels and 6 cases had low folic acid levels. Serum LDH levels were elevated in all cases with mean level of 3423 IU/L. There was a significant negative correlation between HB levels and serum LDH levels (r = -.923, p<0.001) a significant positive correlation between MCV and serum LDH levels(r = +0.810, p<0.001). One month after treatment HB levels and MCV improved (mean HB- 10.3g/dl and mean MCV- 88.3fl/l). There was also a significantly fall in the serum levels of LDH 14 days and one month after treatment (p<0.001, p<0.001 respectively).
Conclusion: Serum LDH levelis an important investigation in the diagnosis and in monitoring the response to treatment in megaloblastic anaemia.
Downloads
References
2. Hess B, Gehm E. Lactic acid dehydrogenase in the human blood. KlinWochenschr. 1955; 33(3-4):91-3.[pubmed]
3. Elliott, B. A., and Fleming, A. F. Brit. med. J., 1, 626.Fleming, A. F., and Elliott, B. A. Ibid., 2, 1108.
4. Eivazi ZJ, Dastgiri S, Sanaat Z. Estimation of the diagnostic value of myeloperoxidase index and lactate dehydrogenase in megaloblastic anemia. J Clin Diag Res. 2007; 1(5):380-384.
5. Labhotia M, Shah P K D, Balani V, Gupta A, Saxena A, Sinha H V .Incidence of megaloblastic anemiainIndian adults and role of serum LDH as a diagnostic tool. Indian Journal of Haematology& Blood Transfusion.1994; 12: 113-115.
6. Goldfarb TG, Papp BJ. Excessively high levels of lactic acid dehydrogenase activity in pernicious anemia. Am J Med. 1963; 34:578-622.[pubmed]
7.Gordin R, Eanri TM. Lactic dehydrogenase in vitamin B12 deficiency. Acta Hematol. 1959;21(1):16-22.[pubmed]
8. Emerson PM, Wilkinson JH. Lactate dehydrogenase in the diagnosis and assessment of response to treatment of megaloblastic anemia. Brit J Hematol. 1966; 12(6):678-87.[pubmed]
9. GronvallC. ; On the serum activity.of lactic acid dehydrogenase and phosphohexose isomerase in pernicious and haemolytic anemia, Scand. Journal of Clinical Pathology and LabInvestigation.1961; 1329-60.[pubmed]
10. Premkumar M, N. Gupta, T. Singh, and T. Velpandian. Cobalamin and Folic Acid Status in Relation to the Etiopathogenesis of Pancytopenia in Adults at a Tertiary Care Centre in North India.2012.[pubmed]
11. Gore B.P, Kurundkar G, Bhat S. Retrospective Study of Serum LDH in Megaloblastic Anemia. Indian Journal of Applied Research. 2015; 5:454-55.
12. Winston RM, Warburton FG, Stott A. Enzymatic diagnosis of megaloblastic anemia. Br J Haematol. 1970; 19(5):587-92.[pubmed]
Copyright (c) 2019 Author (s). Published by Siddharth Health Research and Social Welfare Society

This work is licensed under a Creative Commons Attribution 4.0 International License.

 OAI - Open Archives Initiative
OAI - Open Archives Initiative