
A cross sectional study of in-hospital cases of Pediatric Tuberculosis detected by CBNAAT at a tertiary care teaching hospital of Central India.
Abstract
Background: Childhood tuberculosis is difficult in the identification of the organism due to improper sampling as well as low sensitivity of the smear. Newer diagnostic methods like Cartridge based nucleic acid amplification tests (CBNAAT) can rapidly identify Mycobacterium tuberculosis with improved sensitivity over the smear testing.
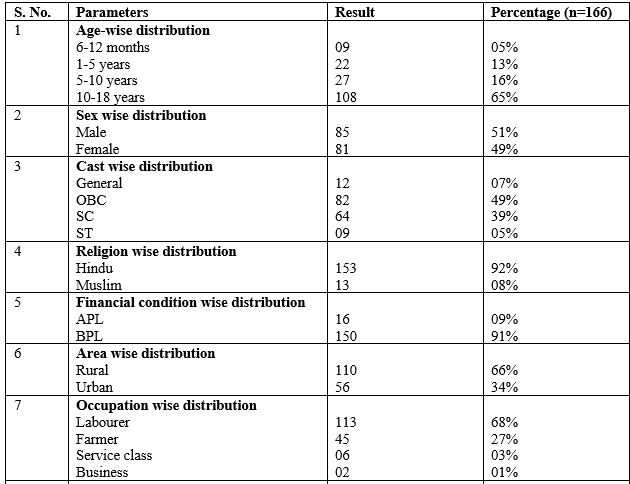
Material & Method: This observational record based cross-sectional study was undertaken to identify the epidemiology of tubercular infection in children diagnosed with CBNAAT. The study was carried out by analyzing the data of children from six months to 18 years who were diagnosed with Tuberculosis and treated with anti-tuberculosis therapy (ATT) from April 2018 to March 2020.
Results: Data of a total of 166 patients was analyzed. 42% of overall collected samples were reactive to CBNAAT testing for tuberculosis. 40 gastric aspirate samples were collected and only four (10%) turned reactive for tuberculosis by CBNAAT. None of the pediatric samples was positive for MDR TB. 66% of children completed treatment and 33% were declared cured.
Conclusion: 42% positivity after CBNAAT testing for tuberculosis infection in collected samples of sputum and gastric aspirate where only 10% yield in GA samples.
Downloads
References
WHO Global Tuberculosis Report 2020.https://www.who.int/teams/global-tuberculosis-programme/data accessed on 07-12-2020
Singh V. Pediatric TB Management Under RNTCP: What and Why? Indian J Pediatr. 2019 Aug;86(8):707-713. DOI: 10.1007/s12098-019-03001-7
Carvalhoa I, Goletti D, Mangac S, Silva DR, et al. Managing latent tuberculosis infection and tuberculosis in children. Pulmonol. 2018; 24(2):106---114. DOI: 10.1016/j.rppnen.2017.10.007
Sahana KS, Prabhu AS, Saldanha PRM. Usage of Cartridge Based Nucleic Acid Amplifification Test (CB-NAAT/GeneXpert) test as diagnostic modality for pediatric tuberculosis; case series from Mangalore, South India. J Clin Tuberc Other Mycobact Dis. 2018; 11:7–9. DOI: 10.1016/j.jctube.2017.12.002
Tuberculosis in Childhood. Delane Shingadia.. Ther Adv Respir Dis 2012: 6(3) 161 –171. https://doi.org/10.1177%2F1753465812436662
https://tbfacts.org/tb-statistics-india/ accessed on 17-06-2020
https://www.who.int/publications/guidelines/en/ accessed on 16-08-2020
https://reports.nikshay.in/Reports/TBNotification accessed on 16-08-2020
Belgaumkar V, Chandanwale A, Valvi C et al. Barriers to screening and isoniazid preventive therapy for child contacts of tuberculosis patients. Int J Tuberc Lung Dis. 2018. 1;22(10):1179-1187. DOI: 10.5588/ijtld.17.0848
Jain SK, Ordonez A, Kinikar A et.al. Pediatric Tuberculosis in Young Children in India: A Prospective Study. BioMed Research International. 2013. https://doi.org/10.1155/2013/783698
Raviglione M., Snider D. , Kochi A. Global epidemiology of tuberculosis JAMA.1995; 273: 220–226. doi:10.1001/jama.1995.03520270054031
Sharma SK, Kohli M, Yadav RN, et al. Evaluating the diagnostic accuracy of xpert MTB/RIF assay in pulmonary tuberculosis. PLoS ONE 2015;10(10). https://doi.org/10.1371/journal.pone.0141011.
Swingler GH, du Toit G, Andronikou S, van der ML, Zar HJ. Diagnostic accuracy of chest radiography in detecting mediastinal lymphadenopathy in suspected pulmonary tuberculosis. Arch Dis Child 2005;90:1153–1156. doi: 10.1136/adc.2004.062315
Zar HJ, Hanslo D, Apolles P, Swingler G, Hussey G. Induced sputum versus gastric lavage for microbiological confirmation of pulmonary tuberculosis in infants and young children: a prospective study. Lancet 2005;365:130–134. doi: 10.1016/S0140-6736(05)17702-2.
Detjen AK, DiNardo AR, Leyden J, Steingart KR, Menzies D, Schiller I, et al. Xpert MTB/RIF assay for the diagnosis of pulmonary tuberculosis in children: a systematic review and meta-analysis. Lancet Respir Med. (2015) 3:451–61. doi: 10.1016/S2213-2600(15)00095-8.
Maciel EL, Brotto LD, Sales CM et al. Gastric lavage in the diagnosis of pulmonary tuberculosis in children: a systematic review. Rev Saúde Pública 2010;44(4). DOI: 10.1590/s0034-89102010005000019
Iram S, Zeenat A, Hussain S, Wasim Yusuf N, Aslam M. Rapid diagnosis of tuberculosis using Xpert MTB/RIF assay Report from a developing country. Pak J Med Sci 2014;31:105 10. DOI: 10.12669/pjms.311.6970
Sharma S, Shulania A, Achra A, et al. Diagnosis of pulmonary tuberculosis from gastric aspirate samples in nonexpectorating pediatric patients in a tertiary care hospital. Indian J Pathol Microbiol 2020;63:210-3.
Copyright (c) 2021 Author (s). Published by Siddharth Health Research and Social Welfare Society

This work is licensed under a Creative Commons Attribution 4.0 International License.

 OAI - Open Archives Initiative
OAI - Open Archives Initiative