
A Clinical, Demographic, Biochemical and Outcome Prole of DiabeticKetoacidosis in Children with Type 1 Diabetes Mellitus
Abstract
Background: Type 1 Diabetes mellitus is one of the most common chronic, endocrine-metabolicsyndrome of children and adolescents. India accounts for most of the children with T1DM in theSoutheast Asia region. The present study was intended to study the clinical, demographic,biochemical and outcome profile of the children admitted with Diabetic ketoacidosis (DKA).
Materialand methods: A prospective, descriptive, observational study was conducted in the PICU tertiarycare hospital over one year. A total of 54 cases admitted of age group 6 months to 14 years withDKA were included and categorized in mild, moderate and severe categories. Various clinical,demographic, biochemical parameters were compared for the association between severity and finaloutcome.
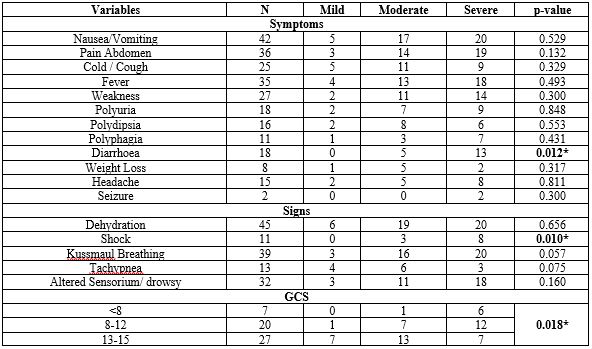
Result: Out of 54 cases admitted with DKA, 39 (72.2%) patients were female, most of thecases belonged to rural areas. Dehydration (83.3%), nausea/vomiting (77.7%), Kussmaul'sbreathing (72.2%) were common presenting symptoms and signs of DKA. The severity of DKA wassignificantly associated with gender, area of residence, socioeconomic status, B.M.I. of the patient,presence of infection, insulin omission, DKA on 1st episode, presence of diarrhea, presence of shock,poor G.C.S. on admission and time required for resolution of DKA (p-value <0.05 for each). Themortality rate was 7.4%.
Conclusion: In our study, the most common precipitating factor observedfor DKA was an infection. For the long-term management strategy, education of the patients andtheir parents regarding infection control, regular blood sugar monitoring and proper Insulin dosingappear to be promising tools.
Downloads
References
2. Van Belle TL, Coppieters KT, Von Herrath MG. Type 1 diabetes: etiology, immunology, and therapeutic strategies. Physiological reviews. 2011 Jan;91(1):79-118. doi.org/10.1152/physrev.00003.2010
3. International Diabetes Federation. IDF Diabetes Atlas, 9th edn. Brussels, Belgium: 2019. Available at: https://www.diabetesatlas.org accessed on 26/10/2020:21:30
4. Zabeen B, Nahar J, Mohsin F, Azad K (2008) DKA in children – An Experience in a Tertiary hospital. Ibrahim Medical Coll J 2: 17-20.
5. Syed M, Khawaja FB, Saleem T, Khalid U, Rashid A, et al. (2011) Clinical profile and outcomes of paediatric patients with diabetic ketoacidosis at a tertiary care hospital in Pakistan. J Pak Med Assoc 61: 1082-1087.
6. Tiwari LK, Jayashree M, Singhi S (2012) Risk factors for cerebral edema in diabetic ketoacidosis in a developing country: role of fluid refractory shock. Pediatr Crit Care Med 13: e91-96
7. Kanwal SK, Bando A, Kumar V (2012) Clinical profile of diabetic ketoacidosis in Indian children. Indian J Pediatr 79: 901-904
8. Basu A, Close CF, Jenkins D, Krentz AJ, Nattrass M, Wright AD. Persisting mortality in diabetic ketoacidosis. Diabet Med 1993; 10: 282-4. 2. doi.org/10.1111/j.1464-5491.1993.tb00060.x
9. Edge JA, Ford-Adams ME, Dunger DB Causes of death in children with insulin dependent diabetes 1990–96 Archives of Disease in Childhood 1999;81:318-323. dx.doi.org/10.1136/adc.81.4.318
10. Bui TP, Werther GA, Cameron FJ. Trends in diabetic ketoacidosis in childhood and adolescence: a 15-year experience. Paediatr Diabetes 2002; 3: 82-8. doi.org/10.1034/j.1399-5448.2002.30204.x
11. Abbas Q, Arbab S, Ul Haque A, Humayun KN. Spectrum of complications of severe DKA in children in pediatric Intensive Care Unit. Pakistan journal of medical sciences. 2018 Jan;34 (1):106. doi: 10.12669/pjms.341.13875
12. Edge JA, Jakes RW, Roy Y, Hawkins M, Winter D, Ford-Adams ME, Murphy NP, Bergomi A, Widmer B, Dunger DB. The UK case–control study of cerebral oedema complicating diabetic ketoacidosis in children. Diabetologia. 2006 Sep 1;49(9):2002-9. DOI: 10.1007/s00125-006-0363-8
13. Ameyaw E, Asafo-Agyei SB, Thavapalan S, Middlehurst AC, Ogle GD. Clinical profile of diabetes at diagnosis among children and adolescents at an endocrine clinic in Ghana. 79 World JDiabetes 2017; 8(9): 429-435.DOI: http://dx.doi.org/10.4239/wjd.v8.i9.429
14. Al Shaikh A, Farahat F, Saeedi M, Bakar A, Al Gahtani A, Al-Zahrani N, Jaha L, Aseeri MA, Al-Jifree HM, Al Zahrani A. Incidence of diabetic ketoacidosis in newly diagnosed type 1 diabetes children in western Saudi Arabia: 11-year experience. Journal of Pediatric Endocrinology and Metabolism. 2019 Aug 27;32 (8):857-62.
15. Basavanthappa SP, Pejaver R, Raghavendra K, Srinivasa V, Suresh Babu MT. Clinical profile and outcome of diabetic ketoacidosis in a tertiary care hospital in South India. Int 80 J Contemp Pediatr. 2015 Jan; 2:29-31.
16. Padma BK, Deepa. (2019). Clinico-laboratory characteristics and immediate outcome in children with diabetes mellitus. Journal of Evolution of Medical and Dental Sciences. 8. 1998-2001. 10.14260/jemds/2019/43
17. Rashid I, Amin A, Mushtaq H & Masood M (2019). Diabetic ketoacidosis and its outcome in children. Asian journal of multidisciplinary studies, 8(1).
18. Ababulgu RZ, Tesfaye BT. Characteristics and Outcomes of Children with Type-I Diabetes Mellitus Hospitalized for Ketoacidosis. Curr Diabetes Rev. 2020;16 (7):779- 786. doi:10.2174/1573399815666190906152125
19. Satti SA, Saadeldin IY, Dammas AS. Diabetic ketoacidosis in children admitted to Pediatric Intensive Care Unit of King Fahad hospital, Al-Baha, Saudi Arabia: precipitating factors, epidemiological parameters and clinical presentation. Sudanese journal of paediatrics. 2013;13 (2):24
20. Bhardwaj P, Yadav V, Sharma M. Clinical profile and outcome of the children with diabetic ketoacidosis (DKA) in hilly Himalayan state of north India. Int J Res Med Sci. 2017;5 (12):5402-5.
21. Kumar MV, Manjusha K. Precipitating factors, clinical profile and metabolic abnormalities of diabetic ketoacidosis in children with type 1 diabetes and their role in predicting the outcome. J Evid Based Med Healthc. 2017;4 (8):393-400
22. Neu A, Ehehalt S, Willasch A, Kehrer M, Hub R, Ranke MB (2001) Varying clinical presentations at onset of type 1 diabetes mellitus in children–epidemiological evidence for different subtypes of the disease? Pediatr Diabetes 2:157–53
23. Islam R, Akhter S, Shelim R, Mohsin F, Begum T, Akhter G. Precipitating factors, clinical features and outcome of diabetic ketoacidosis in children and adolescents admitted in a tertiary care hospital in Dhaka. Bangladesh Journal of Medical Science. 2014;13 (1):53-7.
24. Jayashree M, Singhi S. Diabetic ketoacidosis: predictors of outcome in a pediatric intensive care unit of a developing country. Pediatr Crit Care Med. 2004; 5:427–433. 29.
25. Mbugua PK, Otieno CF, Kayima JK, Amayo AA, McLigeyo SO. Diabetic ketoacidosis: Clinical presentation and precipitating factors at Kenyatta National Hospital, Nairobi. East Afr Med J. 2005;82 (12 Suppl): S191–6
26. Varshney GA, Varshney D, Mehr V, Kela G, Kharia R, Agrawal G, Gupta R. Clinical profile and outcome of diabetic ketoacidosis in children at tertiary care hospital. Journal of Evolution of Medical and Dental Sciences. 2015 Apr 16;4 (31):5329-34.

 OAI - Open Archives Initiative
OAI - Open Archives Initiative