
A study of causes of respiratory distress in neonates presenting within 72 hours
Abstract
Objectives: to determine the prevalence of known causes of respiratory distress (RD) in neonates within 72 hours and their immediate clinical outcome.
Material and methods: All inborn and out born neonates admitted in Neonatal Unit of Pediatric Department of BRD medical College, Gorakhpur who developed RD within 72 hours of life were studied. Neonates with birth weight less than 1000 grams and less than 28 wks of gestation were excluded from the study.
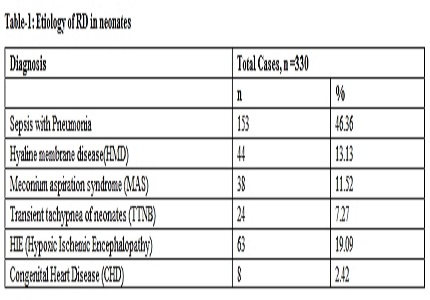
Result: Out of 1032 neonates screened, 330 neonates (31.98%) admitted with features of RD. Male neonates were two third (67.88%) with M: F ratio of 2.1: 1 and two third of them preterm. Sepsis with pneumonia was found to be the most common cause of RD in neonates (46.36%) followed by hypoxic ischemic encephalopathy (19.09%), hyaline membrane disease(HMD) (13.13%), meconium aspiration syndrome (11.52%), transient tachypnea of neonates (7.27%) and congenital heart disease (2.42%). Eighty five percent neonates were delivered outside, out of these 55.2% were delivered at home by untrained birth attendant. Overall mortality was seen in 31.52%, which was highest in HMD (52.3%) and highest (38.9%) amongst neonates of gestational age < 37 weeks. Two twenty nine (69.39%) neonates of RD were kept on ventilator, out of them 99(30.0%) expired, maximum mortality was seen in HMD.
Conclusion: Sepsis with pneumonia was the common cause of admission with features of RD. Mostly these neonates were preterm, delivered outside mainly at home, weighing <2500gm with common responsible organism was Klebsiela. Highest mortality was seen in HMD.
Downloads
References
2. Thomas S, Verma IC, Singh M, Menon PS. Spectrum of respiratory distress syndrome in the newborn in North India: a prospective study. Indian J Pediatr. 1981 Jan-Feb;48(390):61-5. [PubMed]
3. Singh M. Care of the Newborn. 7th edi. Delhi: Sagar Publication; 2010. Respiratory disorder; p. 275-285.
4. Santosh S, Kumar K, Adarsha E. A Clinical Study of Respiratory Distress In Newborn and its Outcome. Indian Journal of Neonatal Medicine and Research. 2013; 1(1): 2-4.
5. Misra PK. Respiratory distress in newborn. A prospective study. Indian Pediatr. 1987 Jan;24(1):77-80. [PubMed]
6. NNPD network. National Neonatal Perinatal Database. Delhi, India. Report 2002-03.
7. Sachdeva A, Dutta AK, Jain MP. Respiratory distress in newborn: Advance in paediatrics; Medical publisher. 2012: 83-91.
8. Cloherty JP, Eichenwald EC, Hansen AR. The High-Risk Newborn: Anticipation, Evaluation, Management and outcome: Manual of neonatal care. 7th edi. Lippincott Williams and Wilkins; 2012. 74-77 p.
9. Mathur NB, Garg K, Kumar S. Respiratory distress in neonates with special reference to pneumonia. Indian Pediatr. 2002 Jun;39(6):529-37. [PubMed]
10. Haque A, Baki MA, Begum T, Akhter S, Begum S, Nahar N. Etiology of Respiratory Distress in Newborn in BIRDEM. Birdem Medical Journal Vol. 2013; 1(1) :19-22.
11. Bajad M, Goyal S, Jain B. Clinical profile of neonates with respiratory distress. Int J Contemp Pediatr 2016 3:1009-13.
12. Dutta A, Sinhamahapatra . K.T . Spectrum of respiratory distress in newborn: A study from a tertiary care hospital in Kolkata. The Child and newborn, 2011; 15(2): 45- 48.
13. Zaazou M. H, Kamal M M, Ali R M, Hussieny N E, Sayed M E, Descriptive study of cases of respiratory distress in NICU in Ahmed Maher Teaching hospital. Medical Journal Cairo University. 2011; 79(1): 441- 48. [PubMed]
14. Hjalmarson O. Epidemiology and classification of acute, neonatal respiratory disorders. A prospective study. Acta Paediatr Scand. 1981 Nov;70(6):773-83. [PubMed]
15. Khatua SP, Gangwal A, Basu P, Palodhi PK. The incidence and etiology of respiratory distress in newborn. Indian Pediatr. 1979 Dec;16(12):1121-6. [PubMed]
16. Thomas S, Verma IC, Singh M, Menon PS. Spectrum of respiratory distress syndrome in the newborn in North India: a prospective study. Indian J Pediatr. 1981 Jan-Feb;48(390):61-5. [PubMed]
17. Kumar P, Kumar R, Narang A. Spectrum of neonatal respiratory distress at PGI. Bul NNF 1999; 13: 8-11.
18. Rubaltelli FF, Dani C, Reali MF, Bertini G, Wiechmann L, Tangucci M, Spagnolo A. Acute neonatal respiratory distress in Italy: a one-year prospective study. Italian Group of Neonatal Pneumology. Acta Paediatr. 1998 Dec;87(12):1261-8.
19. Duke T. Neonatal pneumonia in developing countries. Arch Dis Child Fetal Neonatal Ed. 2005 May;90(3):F211-9. [PubMed]
20. Misra S, Bhakoo ON, Ayyagiri A, Katariya S. Clinical & bacteriological profile of neonatal pneumonia. Indian J Med Res. 1991 Nov;93:366-70. [PubMed]
21. Singh M. Care of the Newborn. 4th edn. Delhi: Sagar Publications; 1991. Perinatal infection; p.154-176.
22. Helve O., Andresson S., Kirjavainen T. and Pitkanen O.M.Improvement of lung compliance during post natal adaptation correlates with airway sodium transport. American Journal of Respiratory and Critical Care Medicine. 2006; 173: 448-52.
23. Singhi S, Singhi PD. Clinical signs in neonatal pneumonia. Lancet. 1990 Oct 27;336(8722):1072-3. [PubMed]
Copyright (c) 2017 Author (s). Published by Siddharth Health Research and Social Welfare Society

This work is licensed under a Creative Commons Attribution 4.0 International License.

 OAI - Open Archives Initiative
OAI - Open Archives Initiative