
Clinical study of infective endocarditis in children: a 3 years experience from MGM Hospital, Warrangal
Abstract
Background: The impact of endocarditis in childhood accompanies many cardio-vascular disorders. Infective endocarditis (IE) is the most frequently occurring form of endocardium inflammation. Prevailing among the agents are Str. Viridans, Str. Haemoliticus, Staph. Aureus, Staph Epidermidis, Enterococcus, etc.
Objective: This study will explore the outcome of children diagnosed with infective endocarditis for a better guidance in management. Methods: This was a prospective study from warrangal from January 2013 to December 2015. 50 patients with definite IE based on modified Duke’s criteria were recruited into the study. Clinical presentation, risk factors, echocardiography and outcome were obtained.
Results: A total of 50 IE patients were included within the study. The mean age was 6 ± 5.45. Most patients (80.39%) were diagnosed within the first week of admission. Staphylococcus aureas was the most common pathogen (38%) and the mitral valve was predominantly affected (68%). Complication were common and in hospital mortality remains high (27.3%).
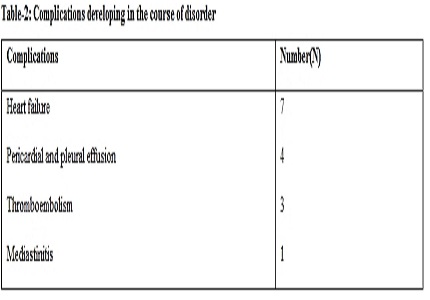
Conclusions: Mortality remains relatively high in children with infective endocarditis. The most common complication is cardiac deficiency (70%), and pleuropericardial effusions and lung embolism
Downloads
References
2. Habib G, Hoen B, Tornos P, Thuny F, Prendergast B, Vilacosta I, Moreillon P, de Jesus Antunes M, Thilen U, Lekakis J, Lengyel M, Müller L, Naber CK, Nihoyannopoulos P, Moritz A, Zamorano JL; ESC Committee for Practice Guidelines. Guidelines on the prevention, diagnosis, and treatment of infective endocarditis (new version 2009): the Task Force on the Prevention, Diagnosis, and Treatment of Infective Endocarditis of the European Society of Cardiology (ESC). Endorsed by the European Society of Clinical Microbiology and Infectious Diseases (ESCMID) and the International Society of Chemotherapy (ISC) for Infection and Cancer. Eur Heart J. 2009 Oct;30(19):2369-413. doi: 10.1093/eurheartj/ehp285. Epub 2009 Aug 27. [PubMed]
3. Zamorano J, Sanz J, Almeria C, Rodrigo JL, Samedi M, Herrera D, et al. Differences between endocarditis with true negative blood cultures and those with previous antibiotic treatment. The Journal of heart valve disease. 2003;12(2):256-60.
4. Jault F, Gandjbakhch I, Rama A, Nectoux M, Bors V, Vaissier E, Nataf P, Pavie A, Cabrol C. Active native valve endocarditis: determinants of operative death and late mortality. Ann Thorac Surg. 1997 Jun;63(6):1737-41. [PubMed]
5. Li JS, Sexton DJ, Mick N, Nettles R, Fowler VG, Jr, Ryan T, et al. Proposed modifications to the Duke criteria for the diagnosis of infective endocarditis. Clin Infect Dis. 2000 Apr;30(4):633-8. Epub 2000 Apr 3. [PubMed]
6. Castillo JC, Anguita MP, Ramirez A, Siles JR, Torres F, Mesa D, et al. Long term outcome of infective endocarditis in patients who were not drug addicts: a 10 year study. Heart. 2000;83(5):525-30. [PubMed]
7. Remadi JP, Habib G, Nadji G, Brahim A, Thuny F, Casalta JP, Peltier M, Tribouilloy C. Predictors of death and impact of surgery in Staphylococcus aureus infective endocarditis. Ann Thorac Surg. 2007 Apr;83(4):1295-302. [PubMed]
8. Bozkurt AK, Oztunc F, Akman C., et al. Multiple pulmonary artery aneurysms due to infective endocarditis. Ann Thorac Surg. 2003 Feb;75(2):593-6. [PubMed]
9. Hufnagel G., Pankuweit S., Richter A., et al. The European Study of Epidemiology and Treatment of Cardiac Inflammatory Diseases (ESETCID). First Epidemiological Results Die European Study of Epidemiology and Treatment of Cardiac Inflammatory Diseases (ESETCID) - Erste epidemiologischemErgebnisse. Herz. 2000; 25: 279-285.
10. Venkatesan C., Wainwright M. Pediatric Endocarditis and Stroke: A Single Center Retrospective Review of SevenCases. Pediatr Neurol. 2008 Apr;38(4):243-7. doi: 10.1016/j.pediatrneurol.2007.12.009.
11. Lertsapcharoen P, Khongphatthanayothin A, Chotivittayatarakorn P, Thisyakorn C, Pathmanand C, Sueblinvong V. Infective endocarditis in pediatric patients: An eighteen-year experience from King Chulalongkorn Memorial Hospital. J Med Assoc Thai. 2005;88(Suppl 4):S12–6. [PubMed]
12. Liew WK, Tan TH, Wong KY..Infective endocarditis in childhood: a seven-year experience. Singapore Med J. 2004 Nov;45(11):525-9. [PubMed]
13. Bitar FF, Jawdi RA, Dbaibo GS, Yunis KA, Gharzeddine W, Obeid M. Paediatric infective endocarditis: 19-year experience at a tertiary care hospital in a developing country. Acta Paediatr. 2000 Apr;89(4):427-30.
14. Coward K, Tucker N, Darville T. Infective endocarditis in Arkansan children from 1990 through 2002. Pediatr Infect Dis J. 2003 Dec;22(12):1048-52. [PubMed]
15. Heper G, Yorukoglu Y. Clinical, bacteriologic and echocardiographic evaluation of infective endocarditis in Ankara, Turkey. Angiology. 2002;53:191–7.
16. Khan NU, Farman MT, Sial JA, Achakzai AS, Saghir T, Ishaq M. Changing trends of infective endocarditis. J Pak Med Assoc. 2010 Jan;60(1):24-7. [PubMed]
17. Tissières P, Gervaix A, Beghetti M, Jaeggi ET. Value and limitations of the von Reyn, Duke, and modified Duke criteria for the diagnosis of infective endocarditis in children. Pediatrics. 2003 Dec;112(6 Pt 1):e467. [PubMed]
18. Lamas CC, Eykyn SJ. Blood culture negative endocarditis: Analysis of 63 cases presenting over 25 years. Heart. 2003 Mar;89(3):258-62. [PubMed]
19. Pereira CA, Rocio SC, Ceolin MF, Lima AP, Borlot F, Pereira RS, et al. Clinical and laboratory findings in a series of cases of infective endocarditis. J Pediatr (Rio J) 2003;79:423–8. [PubMed]
Copyright (c) 2017 Author (s). Published by Siddharth Health Research and Social Welfare Society

This work is licensed under a Creative Commons Attribution 4.0 International License.

 OAI - Open Archives Initiative
OAI - Open Archives Initiative